- 2 -
Enlarge image
|
INSTRUCTIONS FOR EMPLOYERS FIRST REPORT OF
INJURY OR ILLNESS (DWC FORM-001)
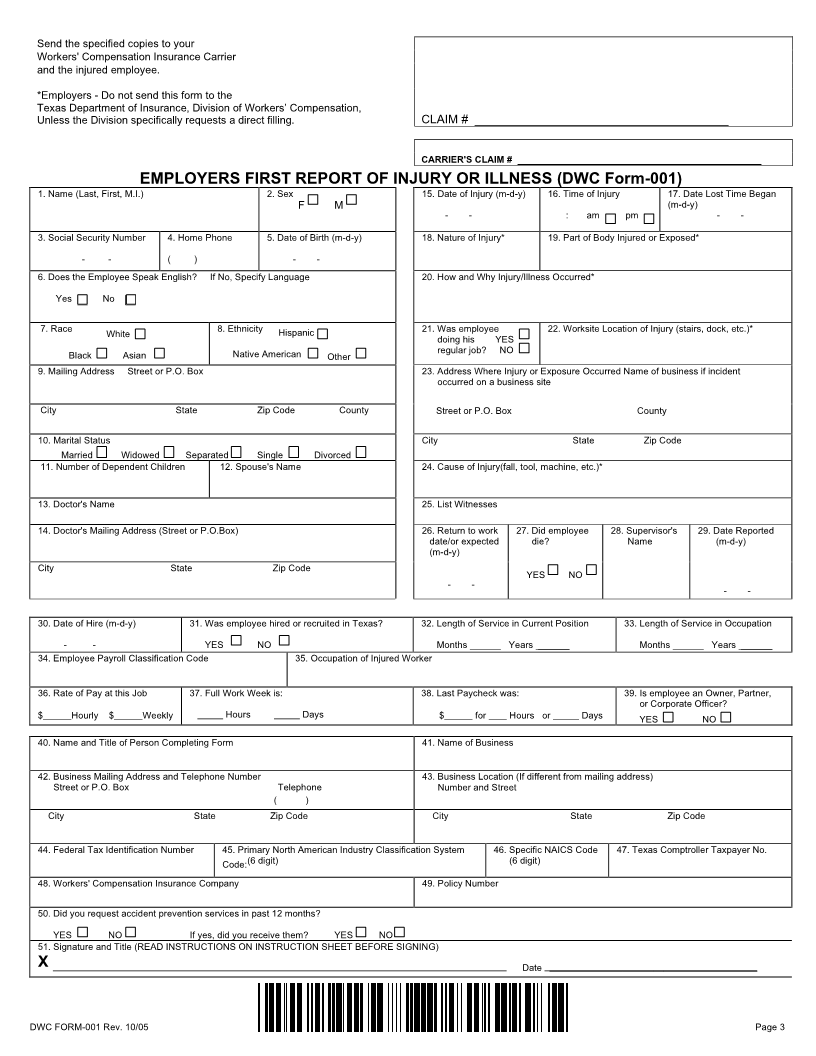
Type (or print in black ink) each item on this form. Failure to complete each item may delay the processing of the injury claim.
Section 409.005, Texas Workers' Compensation Act, requires an Employer's First Report of Injury or Illness (DWC FORM-001 Rev. 10/05 to be
filed with the Workers' Compensation Insurance Carrier not later than the eighth day after the receipt of notice of occupational disease, or the
employee's first day of absence from work due to injury or death. A copy of this report must be sent to the employee or the employee's
representative. For purposes of this section, a report is filed when personally delivered, or postmarked. Send the specified copies to your
Workers' Compensation Insurance Carrier and the injured employee. *Employers - Do not send this form to the Texas Department of
Insurance, Division of Workers' Compensation, unless the Division specifically requests a direct filing.
If a report has not been received by the carrier, the employer has the burden of proving that the report was filed within the required time frame.
The employer has the burden of proving that good cause existed if the employer failed to file the report on time.
An employer who fails to file the report without good cause may be assessed an administrative penalty. An employer who fails to file the report
without good cause waives the right to reimbursement of voluntary benefits even if no administrative penalty is assessed.
Once the employer has completed all information pertaining to the injury the employer should maintain the copy of this report to serve as the
Employer's Record of Injury required by Section 409.006. Send the specified copies to your Workers' Compensation Insurance Carrier and
the injured employee. *Employers - Do not send this form to the Texas Department of Insurance, Division of Workers' Compensation,
unless the Division specifically requests a direct filing. The Division’s Health and Safety will use data from this report for the Job Safety
Information System established in Section 411.032 of the Texas Workers' Compensation Act.
This report may not be considered admission or evidence against the employer or the insurance carrier in any proceeding before the Division or
a court in which facts set out in the report are contradicted by the employer or insurance carrier.
"SPECIAL INSTRUCTIONS FOR CERTAIN ITEMS"
Items 2,7,8: Section 402.082, Texas Workers' Compensation Act requires the Division to maintain information as to the race, ethnicity and
sex on every compensable injury. This information will be maintained for non-discriminatory statistical use.
Item 4: If no home phone, please provide a phone number where the employee can be reached.
Items 5,15,17,
26,29,30: Enter data in month, day, year format. Example: 08-13-54.
Item 18: List nature of accident or exposure, e.g., fall from scaffold, contact with radiation, etc. If occupational disease, so state.
Item 19: List specific body part, e.g., chin, right leg, forehead, left upper arm, etc. If more than one body part is affected, list each part.
Item 20: Describe in detail (1) the events leading up to the injury/illness, (2) the actual injury, e.g., cut left forearm, broken right foot,
etc., and (3) the reason(s) why accident/injury occurred. Use an additional sheet of paper if necessary.
Item 22: State the exact work-site location of the injury, e.g., construction site, office area, storage area, etc.
Item 24: List object, substance, or exposure that directly inflicted the injury or illness, e.g., floor, hammer, chemicals, etc.
Items 32,33: Enter date in month-year format. Example: 02-56.
Item 37: Enter the number of days or hours that make up a full work week for your employees.
Item 45: Enter the 6-digit North American Industry Classification System (NAICS) Code of the employer. The primary code is the code
which appears in block 5 of Form C-3, "Employer's Quarterly Report" to the Texas Workforce Commission.
Item 46: For companies with a single NAICS code, the specific code is the same as the primary code. For companies with multiple
NAICS codes, enter the code that identifies the specific business, activity, or work-site location the employee was working in
at the time of the injury. This may or may not be the same as the primary code.
Note: With few exceptions, on your request, you are entitled to:
• be informed about the information DWC collects about you;
• receive and review the information (Government Code Sections 552.021 and 552.023); and
• have DWC correct information that is incorrect (Government Code Section 559.004).
For more information, contact DWCLegalServices@tdi.texas.gov or refer to the Corrections Procedure section
at www.tdi.texas.gov/commissioner/legal/lccorprc.html.
DWC FORM-001 Rev. 10/05 Page 2
|