Enlarge image
01
0000000000111111111122222222223333333333444444444455555555556666666666777777777788888
1234567890123456789012345678901234567890123456789012345678901234567890123456789012345
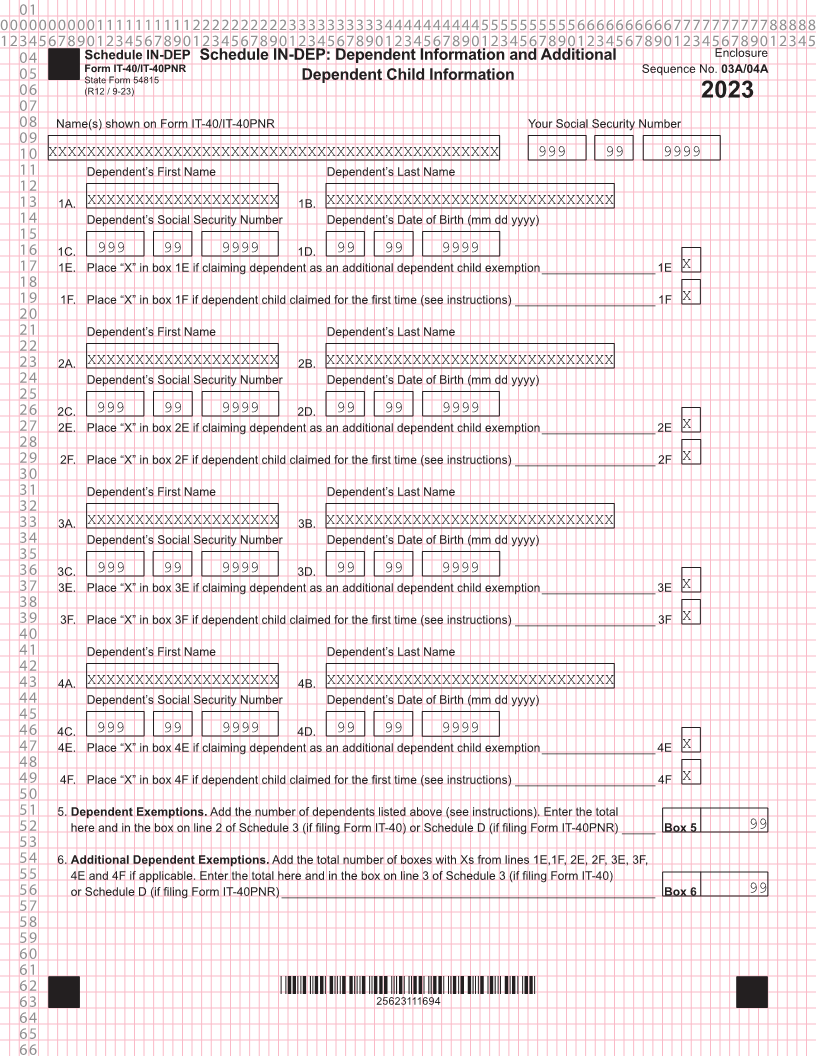
04 Schedule IN-DEP Schedule IN-DEP: Dependent Information and Additional Enclosure
Form IT-40/IT-40PNR Sequence No. 03A/04A
05 State Form 54815 Dependent Child Information
06 (R12 / 9-23)
2023
07
08 Name(s) shown on Form IT-40/IT-40PNR Your Social Security Number
09
10 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 999 99 9999
11 Dependent’s First Name Dependent’s Last Name
12
13 1A. XXXXXXXXXXXXXXXXXXXX 1B. XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
14 Dependent’s Social Security Number Dependent’s Date of Birth (mm dd yyyy)
15
16 1C. 999 99 9999 1D. 99 99 9999
17 1E. Place “X” in box 1E if claiming dependent as an additional dependent child exemption _________________ 1E X
18
19 1F. Place “X” in box 1F if dependent child claimed for the first time (see instructions) _____________________ 1F X
20
21 Dependent’s First Name Dependent’s Last Name
22
23 2A. XXXXXXXXXXXXXXXXXXXX 2B. XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
24 Dependent’s Social Security Number Dependent’s Date of Birth (mm dd yyyy)
25
26 2C. 999 99 9999 2D. 99 99 9999
27 2E. Place “X” in box 2E if claiming dependent as an additional dependent child exemption _________________ 2E X
28
29 2F. Place “X” in box 2F if dependent child claimed for the first time (see instructions) _____________________ 2F X
30
31 Dependent’s First Name Dependent’s Last Name
32
33 3A. XXXXXXXXXXXXXXXXXXXX 3B. XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
34 Dependent’s Social Security Number Dependent’s Date of Birth (mm dd yyyy)
35
36 3C. 999 99 9999 3D. 99 99 9999
37 3E. Place “X” in box 3E if claiming dependent as an additional dependent child exemption _________________ 3E X
38
39 3F. Place “X” in box 3F if dependent child claimed for the first time (see instructions) _____________________ 3F X
40
41 Dependent’s First Name Dependent’s Last Name
42
43 4A. XXXXXXXXXXXXXXXXXXXX 4B. XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
44 Dependent’s Social Security Number Dependent’s Date of Birth (mm dd yyyy)
45
46 4C. 999 99 9999 4D. 99 99 9999
47 4E. Place “X” in box 4E if claiming dependent as an additional dependent child exemption _________________ 4E X
48
49 4F. Place “X” in box 4F if dependent child claimed for the first time (see instructions) _____________________ 4F X
50
51 5. Dependent Exemptions. Add the number of dependents listed above (see instructions). Enter the total
52 here and in the box on line 2 of Schedule 3 (if filing Form IT-40) or Schedule D (if filing Form IT-40PNR) _____ Box 5 99
53
54 6. Additional Dependent Exemptions. Add the total number of boxes with Xs from lines 1E,1F, 2E, 2F, 3E, 3F,
55 4E and 4F if applicable. Enter the total here and in the box on line 3 of Schedule 3 (if filing Form IT-40)
56 or Schedule D (if filing Form IT-40PNR) ________________________________________________________ Box 6 99
57
58
59
60
61
62 *25623111694*
63 25623111694
64
65
66