Enlarge image
Clear Form
Tax Year IT AR
Rev. 9/19
2019
10211411
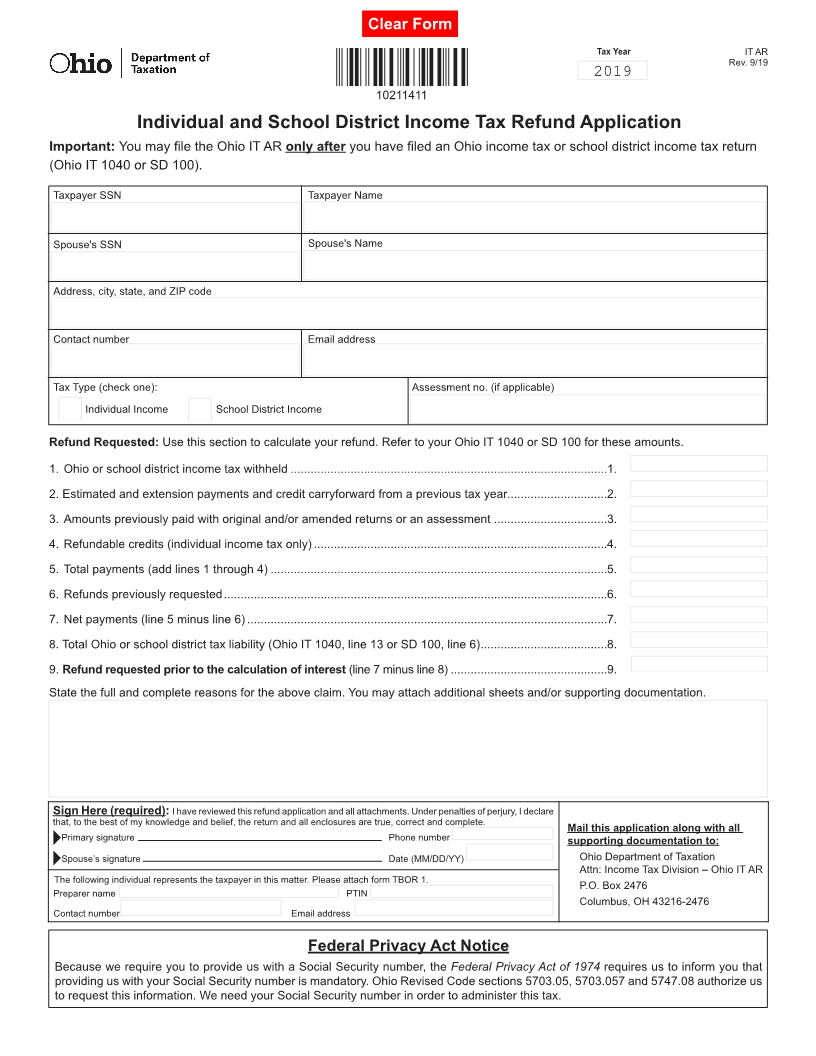
Individual and School District Income Tax Refund Application
Important: You may file the Ohio IT AR only after you have filed an Ohio income tax or school district income tax return
(Ohio IT 1040 or SD 100).
Taxpayer SSN Taxpayer Name
Spouse's SSN Spouse's Name
Address, city, state, and ZIP code
Contact number Email address
Tax Type (check one): Assessment no. (if applicable)
Individual Income School District Income
Refund Requested: Use this section to calculate your refund. Refer to your Ohio IT 1040 or SD 100 for these amounts.
1. Ohio or school district income tax withheld ...............................................................................................1.
2. Estimated and extension payments and credit carryforward from a previous tax year..............................2.
3. Amounts previously paid with original and/or amended returns or an assessment ..................................3.
4. Refundable credits (individual income tax only) ........................................................................................4.
5. Total payments (add lines 1 through 4) .....................................................................................................5.
6. Refunds previously requested ...................................................................................................................6.
7. Net payments (line 5 minus line 6) ............................................................................................................7.
8. Total Ohio or school district tax liability (Ohio IT 1040, line 13 or SD 100, line 6) ......................................8.
9. Refund requested prior to the calculation of interest (line 7 minus line 8) ...............................................9.
State the full and complete reasons for the above claim. You may attach additional sheets and/or supporting documentation.
Sign Here (required): I have reviewed this refund application and all attachments. Under penalties of perjury, I declare
that, to the best of my knowledge and belief, the return and all enclosures are true, correct and complete.
Mail this application along with all
Primary signature Phone number supporting documentation to:
Spouse’s signature Date (MM/DD/YY) Ohio Department of Taxation
Attn: Income Tax Division – Ohio IT AR
The following individual represents the taxpayer in this matter. Please attach form TBOR 1. P.O. Box 2476
Preparer name PTIN
Columbus, OH 43216-2476
Contact number Email address
Federal Privacy Act Notice
Because we require you to provide us with a Social Security number, the Federal Privacy Act of 1974 requires us to inform you that
providing us with your Social Security number is mandatory. Ohio Revised Code sections 5703.05, 5703.057 and 5747.08 authorize us
to request this information. We need your Social Security number in order to administer this tax.