Enlarge image
DTE 105H
Rev. 10/19
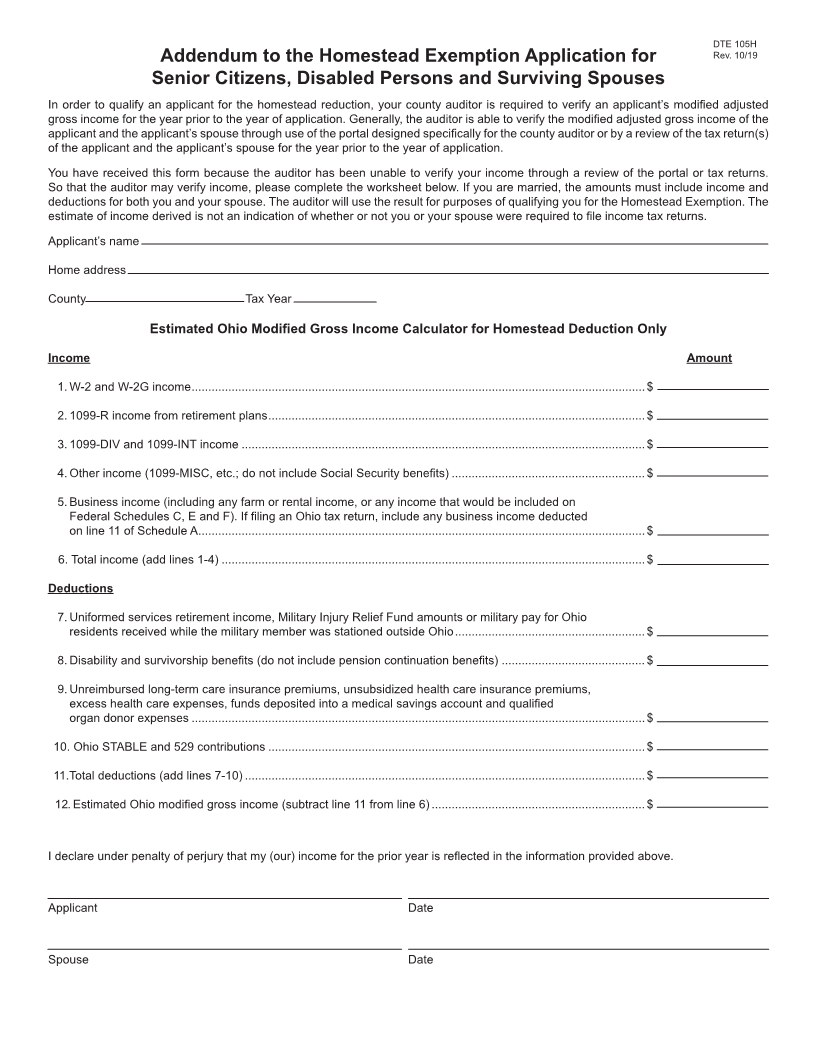
Addendum to the Homestead Exemption Application for
Senior Citizens, Disabled Persons and Surviving Spouses
In order to qualify an applicant for the homestead reduction, your county auditor is required to verify an applicant’s modified adjusted
gross income for the year prior to the year of application. Generally, the auditor is able to verify the modified adjusted gross income of the
applicant and the applicant’s spouse through use of the portal designed specifically for the county auditor or by a review of the tax return(s)
of the applicant and the applicant’s spouse for the year prior to the year of application.
You have received this form because the auditor has been unable to verify your income through a review of the portal or tax returns.
So that the auditor may verify income, please complete the worksheet below. If you are married, the amounts must include income and
deductions for both you and your spouse. The auditor will use the result for purposes of qualifying you for the Homestead Exemption. The
estimate of income derived is not an indication of whether or not you or your spouse were required to file income tax returns.
Applicant’s name
Home address
County Tax Year
Estimated Ohio Modified Gross Income Calculator for Homestead Deduction Only
Income Amount
1. W-2 and W-2G income ........................................................................................................................................$
2. 1099-R income from retirement plans .................................................................................................................$
3. 1099-DIV and 1099-INT income .........................................................................................................................$
4. Other income (1099-MISC, etc.; do not include Social Security benefits) ..........................................................$
5. Business income (including any farm or rental income, or any income that would be included on
Federal Schedules C, E and F). If filing an Ohio tax return, include any business income deducted
on line 11 of Schedule A ......................................................................................................................................$
6. Total income (add lines 1-4) ...............................................................................................................................$
Deductions
7. Uniformed services retirement income, Military Injury Relief Fund amounts or military pay for Ohio
residents received while the military member was stationed outside Ohio .........................................................$
8. Disability and survivorship benefits (do not include pension continuation benefits) ...........................................$
9. Unreimbursed long-term care insurance premiums, unsubsidized health care insurance premiums,
excess health care expenses, funds deposited into a medical savings account and qualified
organ donor expenses ........................................................................................................................................$
10. Ohio STABLE and 529 contributions .................................................................................................................$
11.Total deductions (add lines 7-10) ........................................................................................................................$
12. Estimated Ohio modified gross income (subtract line 11 from line 6) ................................................................$
I declare under penalty of perjury that my (our) income for the prior year is reflected in the information provided above.
Applicant Date
Spouse Date
