Enlarge image
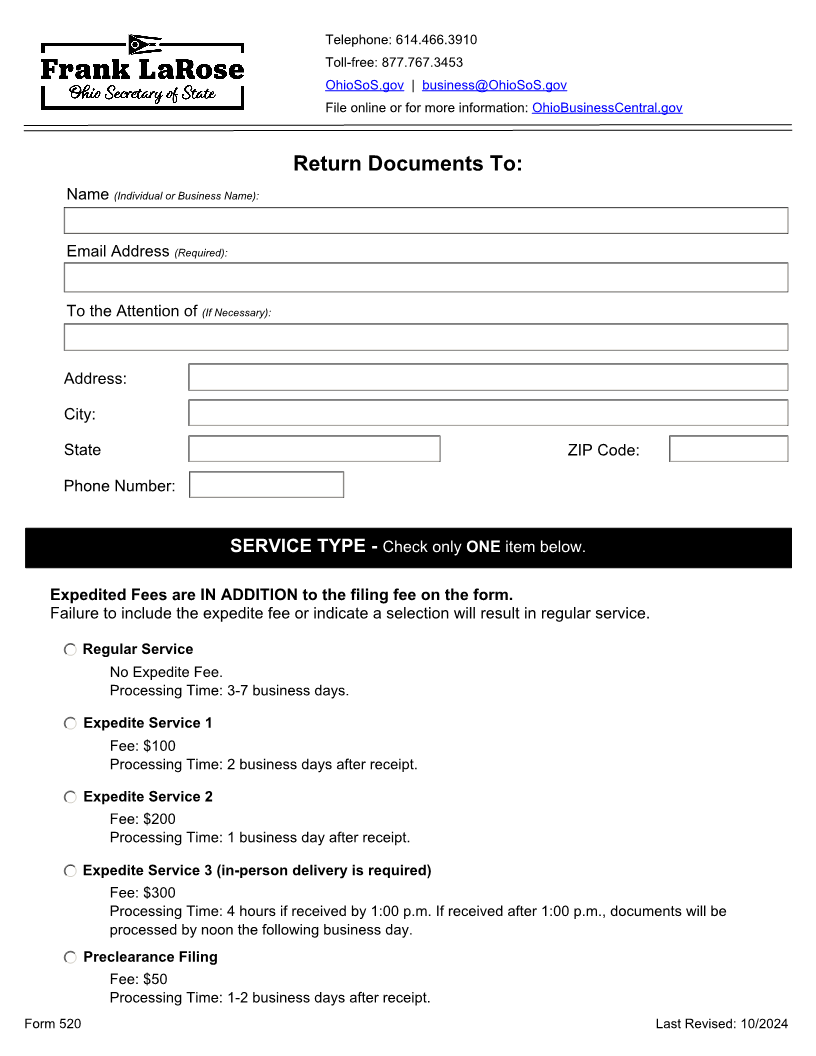
Telephone: 614.466.3910
Toll-free: 877.767.3453
OhioSoS.gov | business@OhioSoS.gov
File online or for more information: OhioBusinessCentral.gov
Return Documents To:
Name (Individual or Business Name):
Email Address (Required):
To the Attention of (If Necessary):
Address:
City:
State ZIP Code:
Phone Number:
SERVICE TYPE - Check only ONE item below.
Expedited Fees are IN ADDITION to the filing fee on the form.
Failure to include the expedite fee or indicate a selection will result in regular service.
Regular Service
· No Expedite Fee.
· Processing Time: 3-7 business days.
Expedite Service 1
· Fee: $100
· Processing Time: 2 business days after receipt.
Expedite Service 2
· Fee: $200
· Processing Time: 1 business day after receipt.
Expedite Service 3 (in-person delivery is required)
· Fee: $300
· Processing Time: 4 hours if received by 1:00 p.m. If received after 1:00 p.m., documents will be
processed by noon the following business day.
Preclearance Filing
· Fee: $50
· Processing Time: 1-2 business days after receipt.
Form 520 Last Revised: 10/2024