- 18 -
Enlarge image
|
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85
2
3
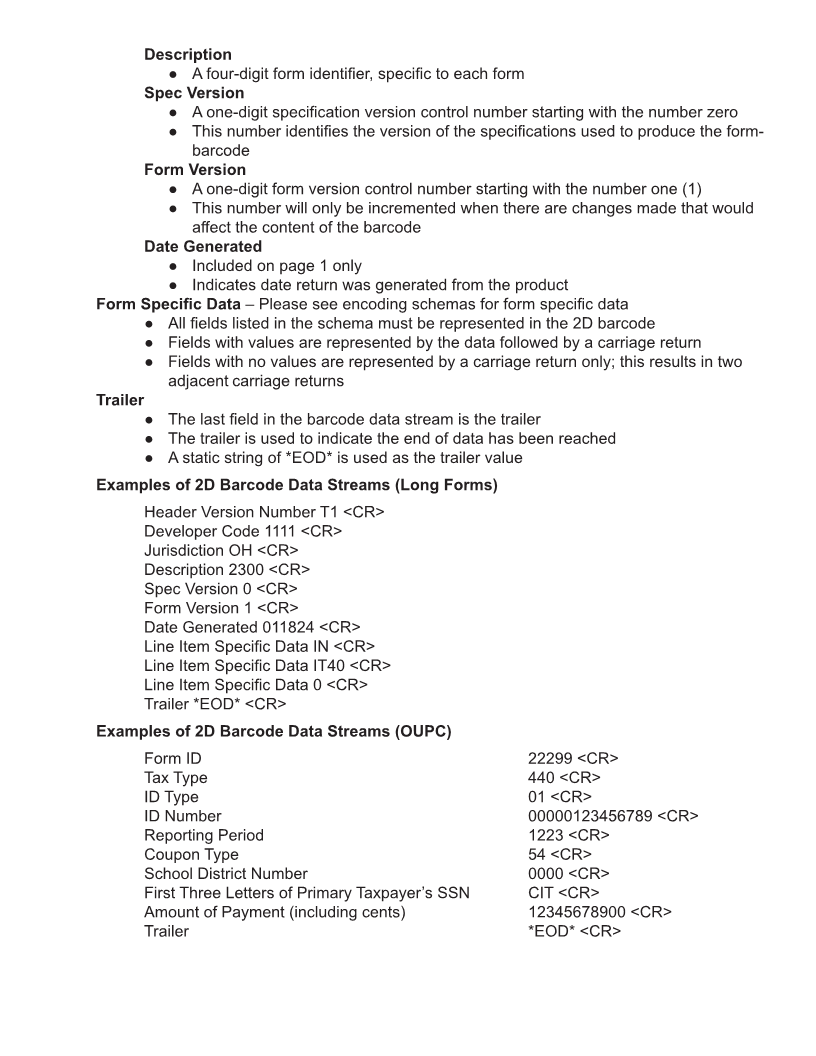
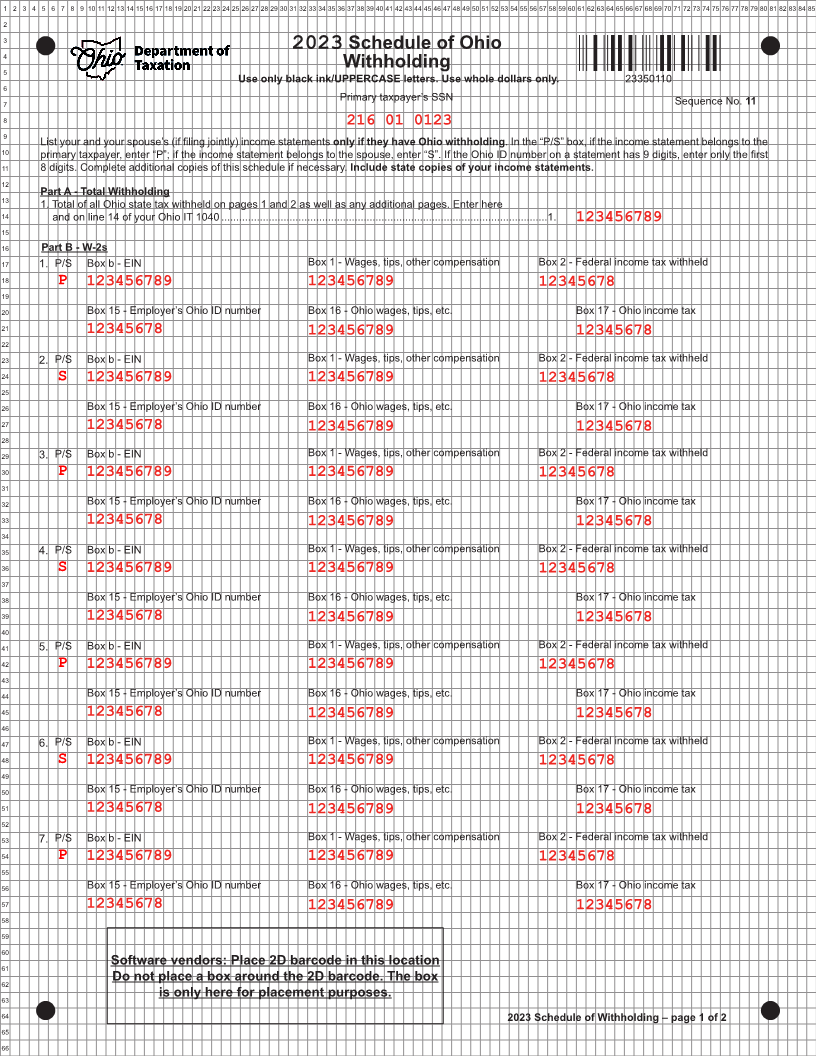
4 2023 Schedule of Ohio
5 Withholding
Use only black ink/UPPERCASE letters. Use whole dollars only. 23350110
6
7 Primary taxpayer’s SSN Sequence No. 11
8
216 01 0123
9
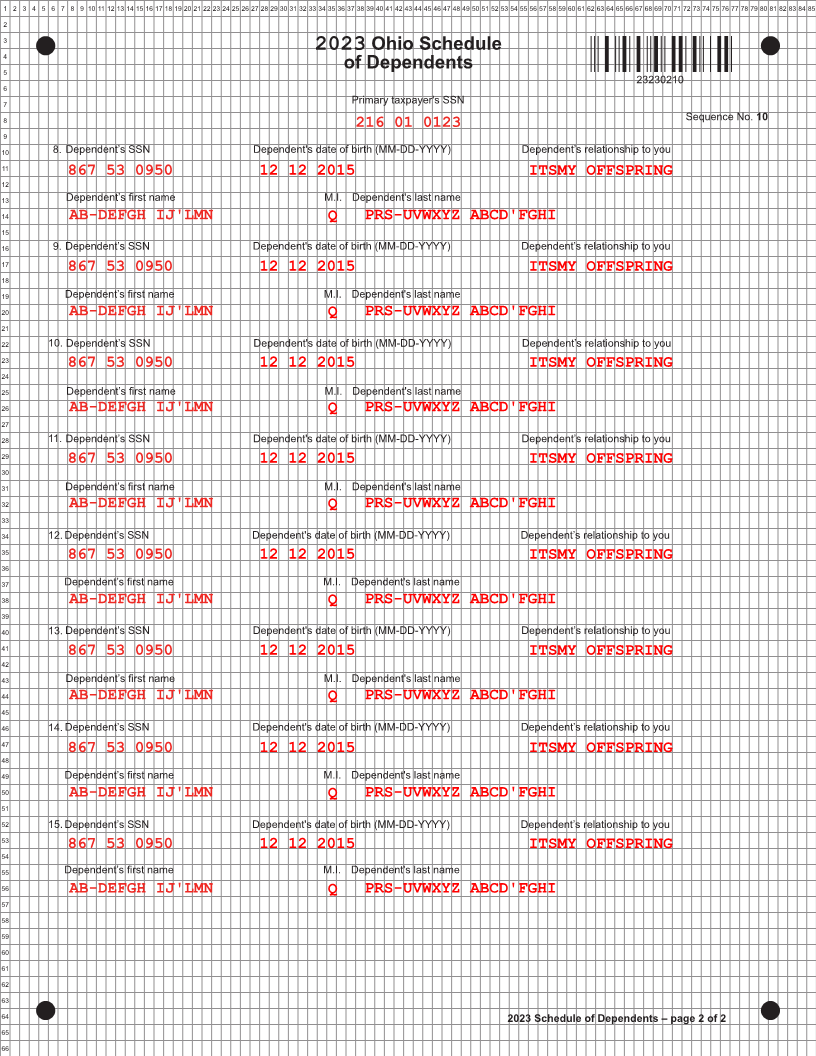
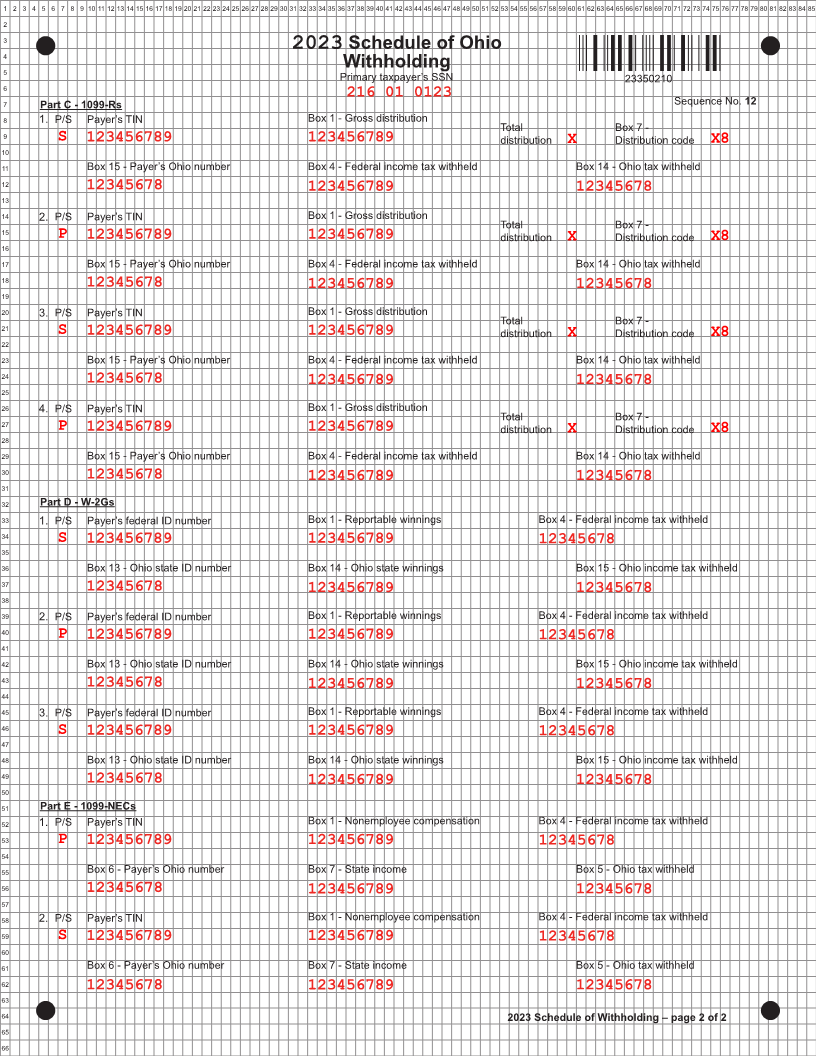
List your and your spouse’s (if filing jointly) income statements only if they have Ohio withholding. In the “P/S” box, if the income statement belongs to the
10 primary taxpayer, enter “P”; if the income statement belongs to the spouse, enter “S”. If the Ohio ID number on a statement has 9 digits, enter only the first
11 8 digits. Complete additional copies of this schedule if necessary. Include state copies of your income statements.
12
13 Part A - Total Withholding
1. Total of all Ohio state tax withheld on pages 1 and 2 as well as any additional pages. Enter here
14 and on line 14 of your Ohio IT 1040 ..............................................................................................................1. 123456789
15
16 Part B - W-2s
17 1. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
18
P 123456789 123456789 12345678
19
20 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
21
22 12345678 123456789 12345678
23 2. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
24
S 123456789 123456789 12345678
25
26 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
27
12345678
28 123456789 12345678
29 3. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
123456789 123456789
30 P 12345678
31
32 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
33
12345678 123456789 12345678
34
35 4. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
123456789 123456789
36 S 12345678
37
38 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
39
12345678 123456789 12345678
40
41 5. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
123456789 123456789
42 P 12345678
43
44 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
45
12345678 123456789 12345678
46
47 6. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
123456789 123456789
48 S 12345678
49
50 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
51
12345678 123456789 12345678
52
53 7. P/S Box b - EIN Box 1 - Wages, tips, other compensation Box 2 - Federal income tax withheld
123456789 123456789
54 P 12345678
55
56 Box 15 - Employer’s Ohio ID number Box 16 - Ohio wages, tips, etc. Box 17 - Ohio income tax
57
12345678 123456789 12345678
58
59
60
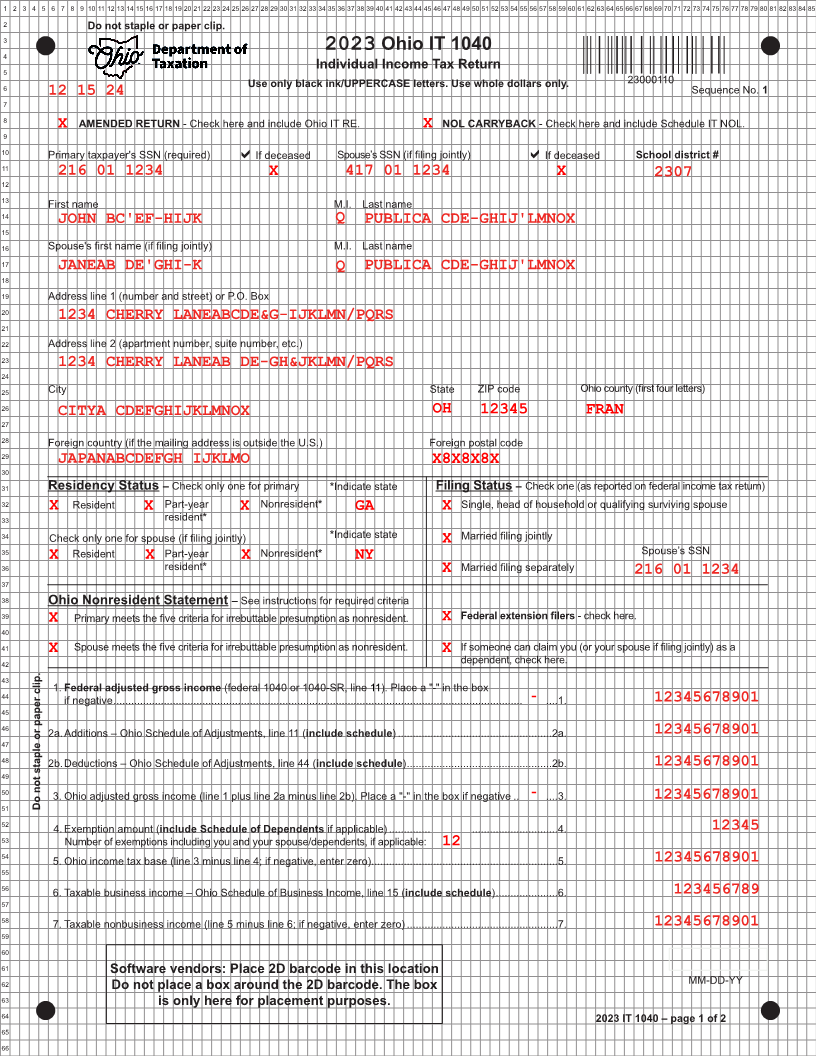
61 Software vendors: Place 2D barcode in this location
62 Do not place a box around the 2D barcode. The box
63 is only here for placement purposes.
64 2023 Schedule of Withholding – page 1 of 2
65
66
|