Enlarge image
Reset Form
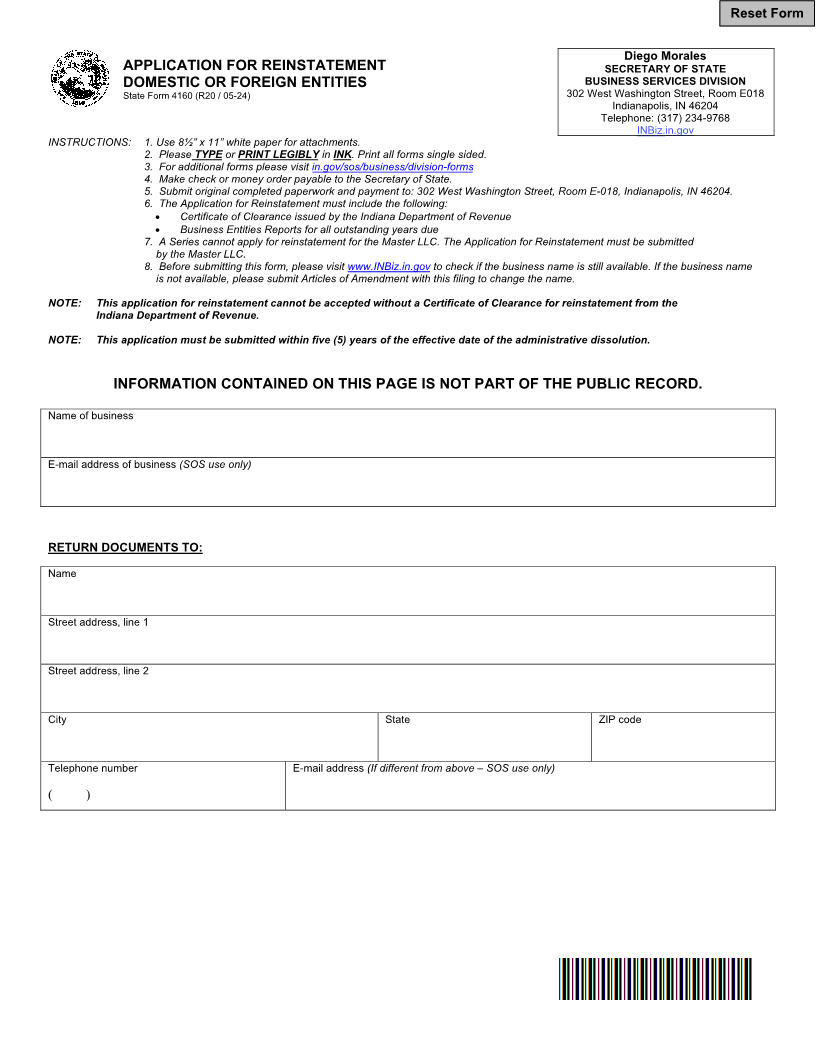
Diego Morales
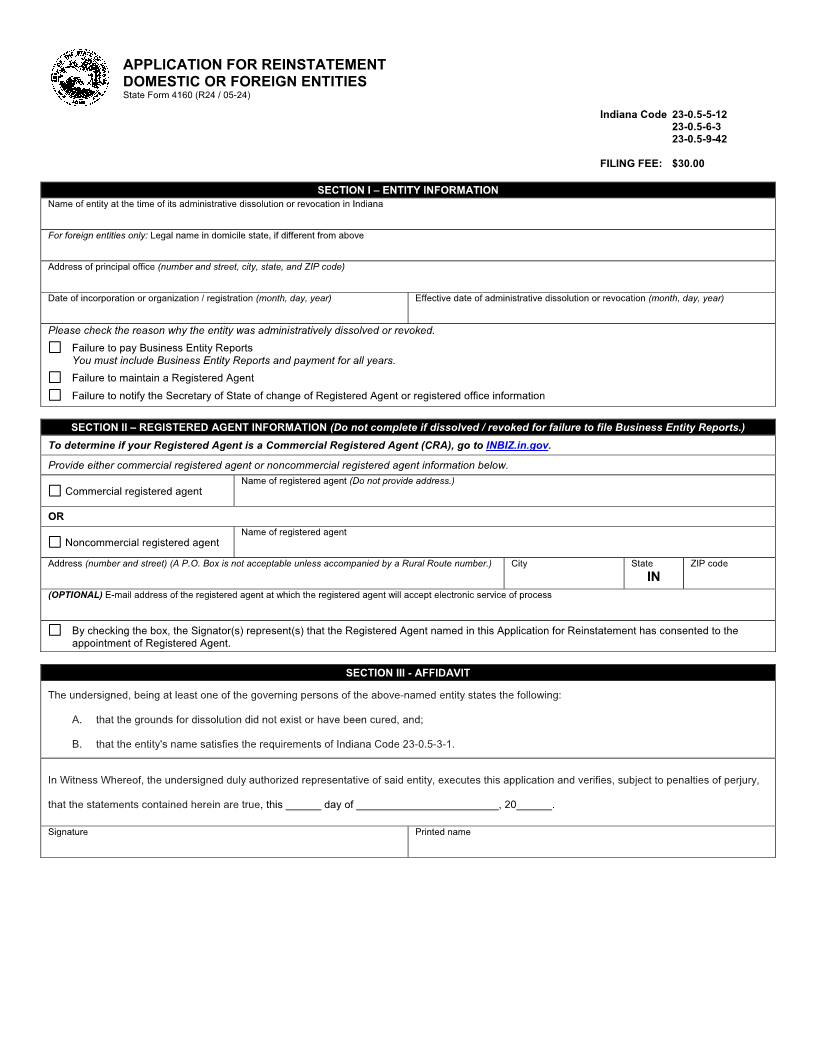
APPLICATION FOR REINSTATEMENT SECRETARY OF STATE
DOMESTIC OR FOREIGN ENTITIES BUSINESS SERVICES DIVISION
State Form 4160 (R20 / 05-24) 302 West Washington Street, Room E018
Indianapolis, IN 46204
Telephone: (317) 234-9768
INBiz.in.gov
INSTRUCTIONS: 1. Use 8½” x 11” white paper for attachments.
2. Please TYPE or PRINT LEGIBLY in INK. Print all forms single sided.
3. For additional forms please visit in.gov/sos/business/division-forms
4. Make check or money order payable to the Secretary of State.
5. Submit original completed paperwork and payment to: 302 West Washington Street, Room E-018, Indianapolis, IN 46204.
6. The Application for Reinstatement must include the following:
•Certificate of Clearance issued by the Indiana Department of Revenue
•Business Entities Reports for all outstanding years due
7. A Series cannot apply for reinstatement for the Master LLC. The Application for Reinstatement must be submitted
by the Master LLC.
8. Before submitting this form, please visit www.INBiz.in.gov to check if the business name is still available. If the business name
is not available, please submit Articles of Amendment with this filing to change the name.
NOTE: This application for reinstatement cannot be accepted without a Certificate of Clearance for reinstatement from the
Indiana Department of Revenue.
NOTE: This application must be submitted within five (5) years of the effective date of the administrative dissolution.
INFORMATION CONTAINED ON THIS PAGE IS NOT PART OF THE PUBLIC RECORD.
Name of business
E-mail address of business (SOS use only)
RETURN DOCUMENTS TO:
Name
Street address, line 1
Street address, line 2
City State ZIP code
Telephone number E-mail address (If different from above – SOS use only)
( )