Enlarge image
Schedule Enclosure
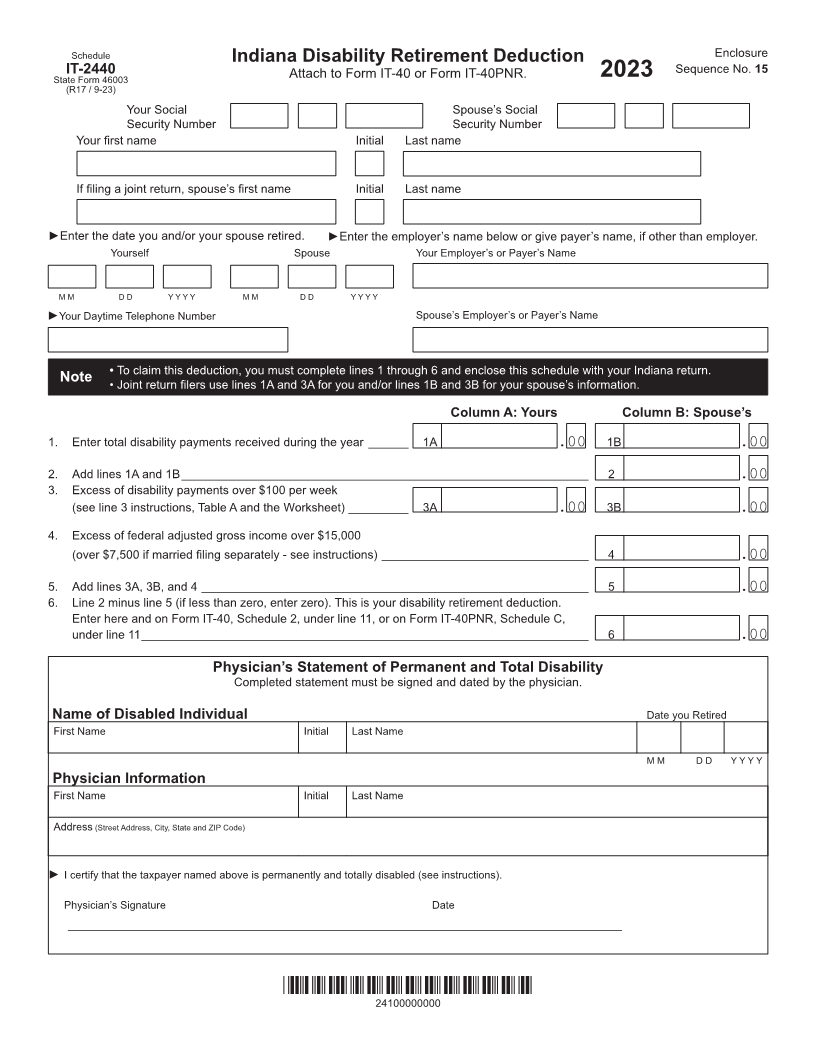
Indiana Disability Retirement Deduction
IT-2440 Attach to Form IT-40 or Form IT-40PNR. Sequence No. 15
State Form 46003 2023
(R17 / 9-23)
Your Social Spouse’s Social
Security Number Security Number
Your first name Initial Last name
If filing a joint return, spouse’s first name Initial Last name
►Enter the date you and/or your spouse retired. ►Enter the employer’s name below or give payer’s name, if other than employer.
Yourself Spouse Your Employer’s or Payer’s Name
M M D D Y Y Y Y M M D D Y Y Y Y
►Your Daytime Telephone Number Spouse’s Employer’s or Payer’s Name
• To claim this deduction, you must complete lines 1 through 6 and enclose this schedule with your Indiana return.
Note • Joint return filers use lines 1A and 3A for you and/or lines 1B and 3B for your spouse’s information.
Column A: Yours Column B: Spouse’s
1. Enter total disability payments received during the year ______ 1A .00 1B .00
2. Add lines 1A and 1B _____________________________________________________________ 2 .00
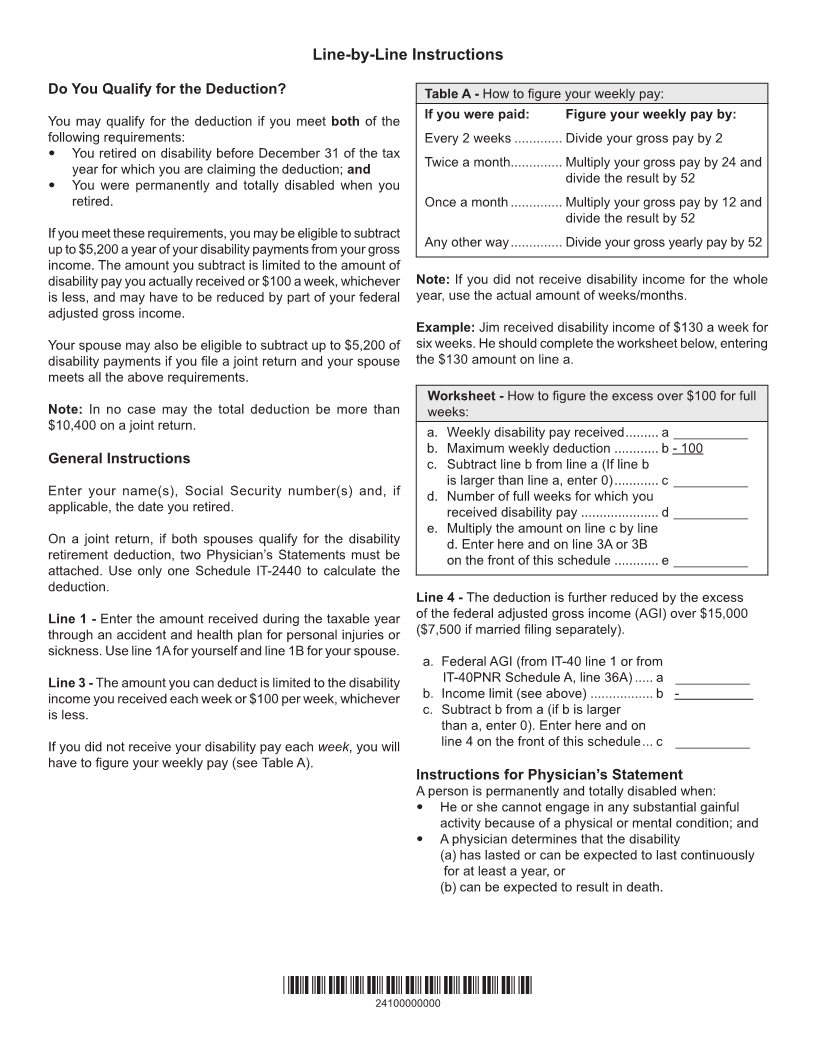
3. Excess of disability payments over $100 per week
(see line 3 instructions, Table A and the orksheet)W _________ 3A .00 3B .00
4. Excess of federal adjusted gross income over $15,000
(over $7,500 if married filing separately - see instructions) _______________________________ 4 .00
5. Add lines 3A, 3B, and 4 __________________________________________________________ 5 .00
6. Line 2 minus line 5 (if less than zero, enter zero). This is your disability retirement deduction.
Enter here and on Form IT-40, Schedule 2, under line 11, or on Form IT-40PNR, Schedule C,
under line 11 ___________________________________________________________________ 6 .00
Physician’s Statement of Permanent and Total Disability
Completed statement must be signed and dated by the physician.
Name of Disabled Individual Date you Retired
First Name Initial Last Name
M M D D Y Y Y Y
Physician Information
First Name Initial Last Name
Address (Street Address, City, State and ZIP Code)
► I certify that the taxpayer named above is permanently and totally disabled (see instructions).
Physician’s Signature Date
___________________________________________________________________________________
*24100000000*
24100000000