Enlarge image
DR-26
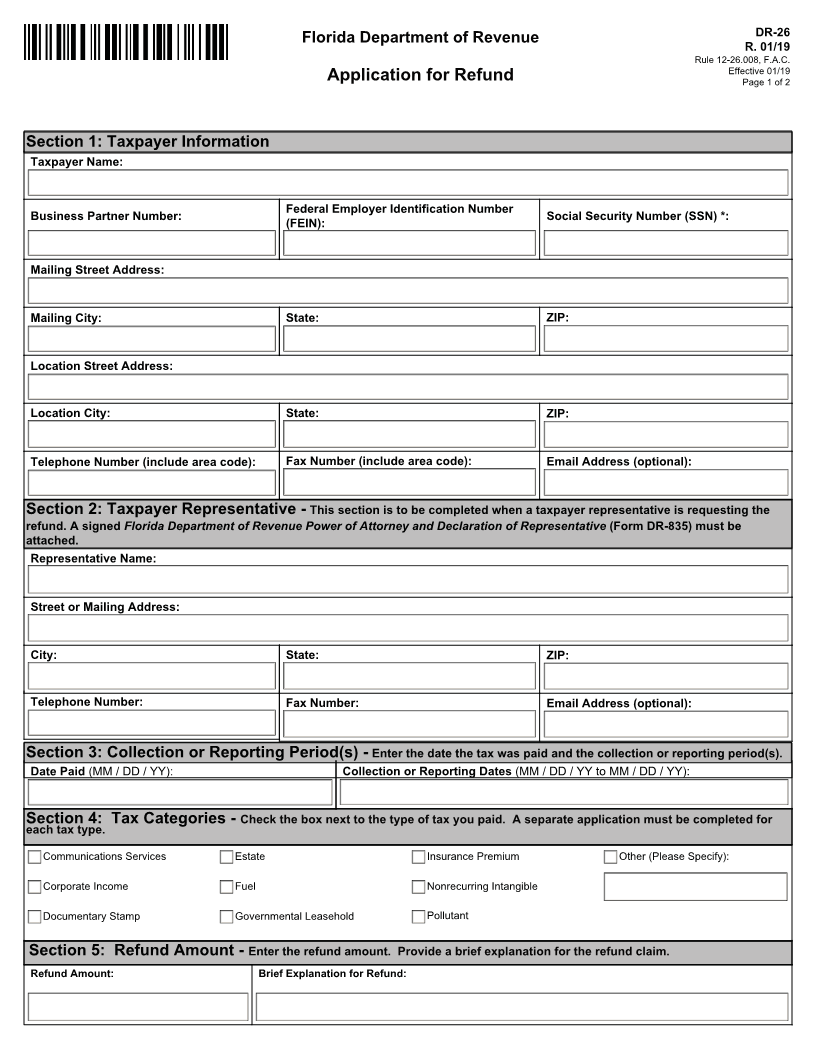
Florida Department of Revenue
R. 01/19
Rule 12-26.008, F.A.C.
Effective 01/19
Application for Refund Page 1 of 2
Section 1: Taxpayer Information
Taxpayer Name:
Federal Employer Identification Number
Business Partner Number: Social Security Number (SSN) *:
(FEIN):
Mailing Street Address:
Mailing City: State: ZIP:
Location Street Address:
Location City: State: ZIP:
Telephone Number (include area code): Fax Number (include area code): Email Address (optional):
Section 2: Taxpayer Representative - This section is to be completed when a taxpayer representative is requesting the
refund. A signed Florida Department of Revenue Power of Attorney and Declaration of Representative (Form DR-835) must be
attached.
Representative Name:
Street or Mailing Address:
City: State: ZIP:
Telephone Number: Fax Number: Email Address (optional):
Section 3: Collection or Reporting Period(s) - Enter the date the tax was paid and the collection or reporting period(s).
Date Paid (MM / DD / YY): Collection or Reporting Dates (MM / DD / YY to MM / DD / YY):
Section 4: Tax Categories - Check the box next to the type of tax you paid. A separate application must be completed for
each tax type.
Communications Services Estate Insurance Premium Other (Please Specify):
Corporate Income Fuel Nonrecurring Intangible
Documentary Stamp Governmental Leasehold Pollutant
Section 5: Refund Amount - Enter the refund amount. Provide a brief explanation for the refund claim.
Refund Amount: Brief Explanation for Refund: