Enlarge image
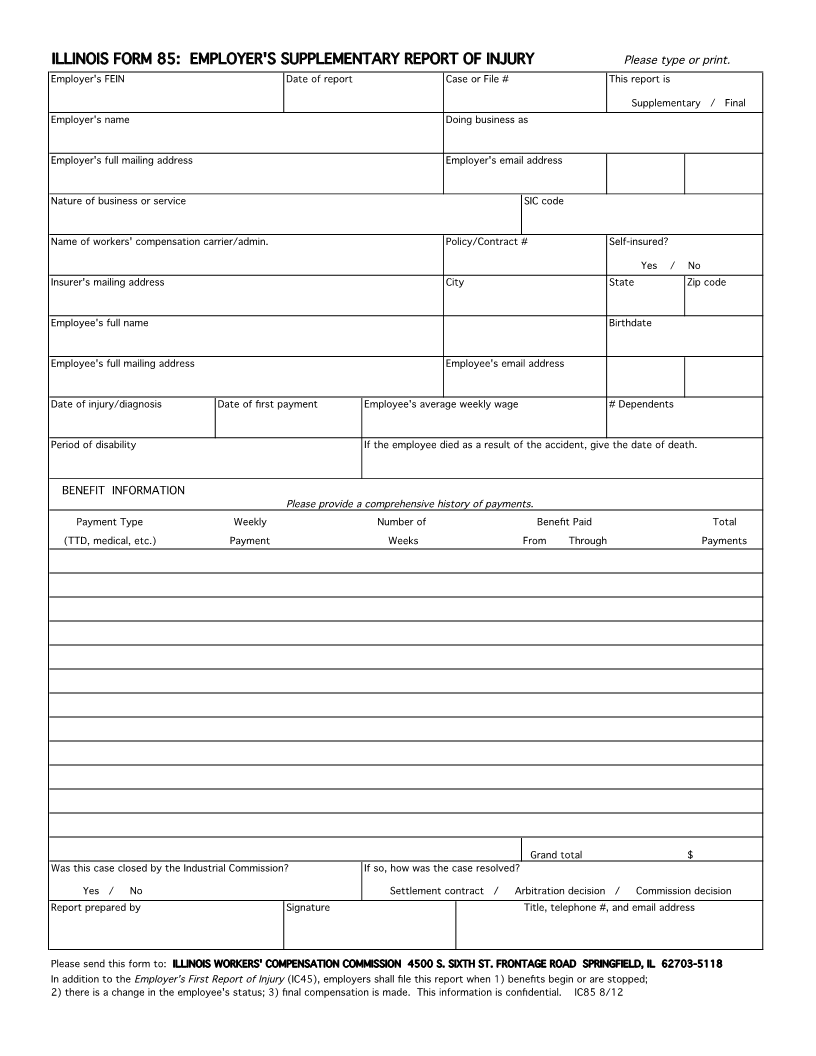
ILLINOIS FORM 85: EMPLOYER'S SUPPLEMENTARY REPORT OF INJURY Please type or print.
Employer's FEIN Date of report Case or File # This report is
Supplementary / Final
Employer's name Doing business as
Employer's full mailing address Employer's email address
Nature of business or service SIC code
Name of workers' compensation carrier/admin. Policy/Contract # Self-insured?
Yes / No
Insurer's mailing address City State Zip code
Employee's full name Birthdate
Employee's full mailing address Employee's email address
Date of injury/diagnosis Date of first payment Employee's average weekly wage # Dependents
Period of disability If the employee died as a result of the accident, give the date of death.
BENEFIT INFORMATION
Please provide a comprehensive history of payments.
Payment Type Weekly Number of Benefit Paid Total
(TTD, medical, etc.) Payment Weeks From Through Payments
Grand total $
Was this case closed by the Industrial Commission? If so, how was the case resolved?
Yes / No Settlement contract / Arbitration decision / Commission decision
Report prepared by Signature Title telephone #, , and email address
Please send this form to: ILLINOIS WORKERS' COMPENSATION COMMISSION 4500 S. SIXTH ST. FRONTAGE ROAD SPRINGFIELD, IL 62703-5118
In addition to the Employer's First Report of Injury (IC45), employers shall file this report when 1) benefits begin or are stopped;
2) there is a change in the employee's status; 3) final compensation is made. This information is confidential. IC85 8/12