Enlarge image
Reset Form
Do not use staples. Use only black ink and UPPERCASE letters.
Depa~ment of 2016 Ohio IT 1040
* Ohio I Taxation
Rev. 9/16 1111111111 1111111 1111111 *
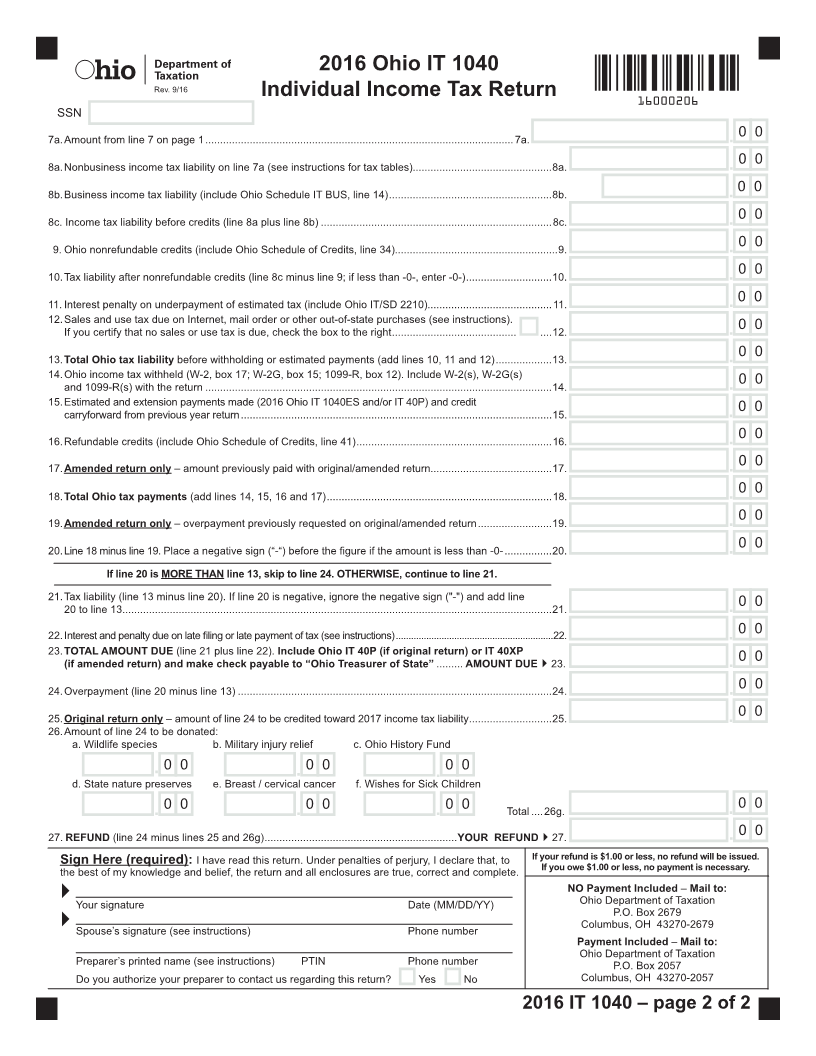
Individual Income Tax Return 16000106
Note: This form encompasses the IT 1040, IT 1040EZ and amended IT 1040X.
Is this an amended return? Yes No If yes, include Ohio IT RE (do not include a copy of the previously filed return)
Is this a Net Operating Loss (NOL) carryback? Yes No If yes, include Schedule IT NOL
Taxpayer's SSN (required) If deceased Spouse’s SSN (if filing jointly) If deceased Enter school district # for
this return (see instructions).
check box check box SD#
First name M.I. Last name
Spouse's fi rst name (only if married filing jointly) M.I. Last name
Mailing address (for faster processing, use a street address)
City State ZIP code Ohio county (fi rst four letters)
Home address (if different from mailing address) – do NOT include city or state ZIP code Ohio county (fi rst four letters)
Foreign country (if the mailing address is outside the U.S.) Foreign postal code
Ohio Residency Status – Check applicable box Filing Status – Check one (as reported on federal income tax return,
Full-year Part-year Nonresident with limited exceptions – see instructions)
resident resident Indicate state
Single, head of household or qualifying widow(er)
Check applicable box for spouse (only if married filing jointly)
Full-year Part-year Nonresident Married filing jointly Married filing separately
Yes No
resident resident Indicate state
Yes No Did you fi le the federal extension 4868? ......................................
Ohio Political Party Fund Yes No
Do you want $1 to go to this fund?............................................ Is someone else claiming you or your spouse (if joint return) as
a dependent? If yes, enter "0" on line 4........................................
If joint return, does your spouse want $1 to go to this fund?.....
Note: Checking “Yes” will not increase your tax or decrease your refund.
1. Federal adjusted gross income (from the federal 1040, line 37; 1040A, line 21; 1040EZ,
line 4; 1040NR, line 36; or 1040NR-EZ, line 10). Place a negative sign (“-“) before the figure if
the amount is less than -0-...................................................................................................................1. . 00
00
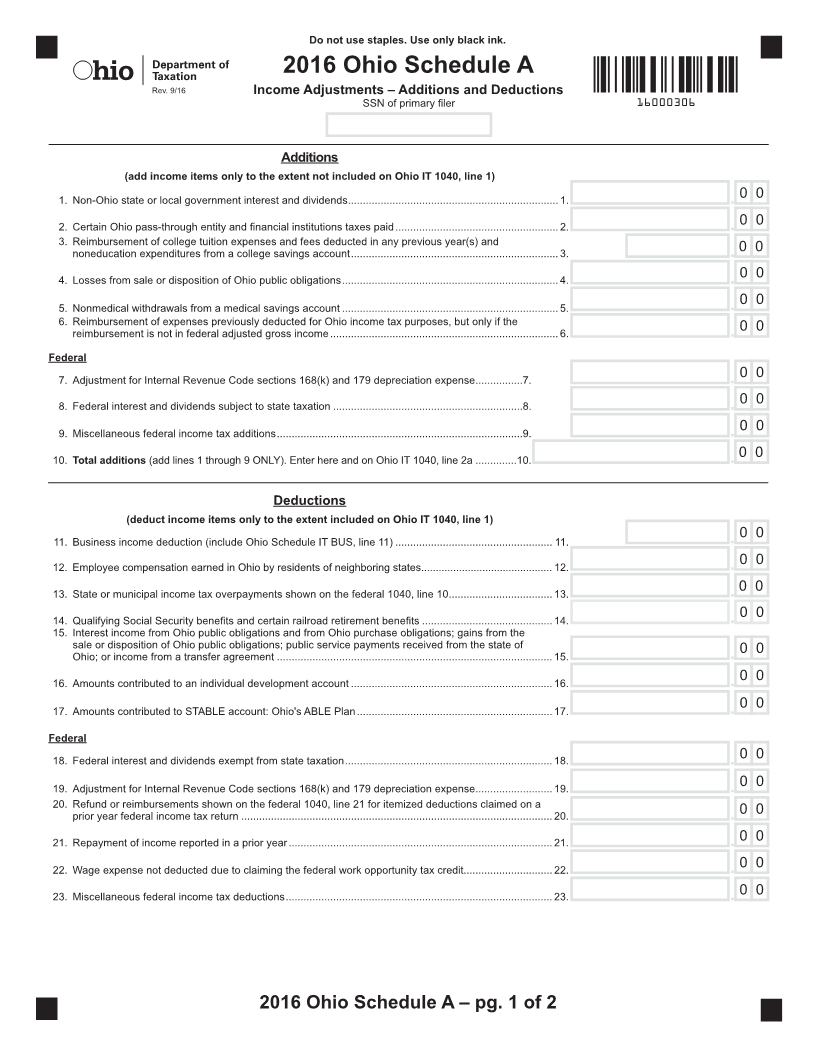
2a.Additions to federal adjusted gross income (include Ohio Schedule A, line 10) ............................2a. .
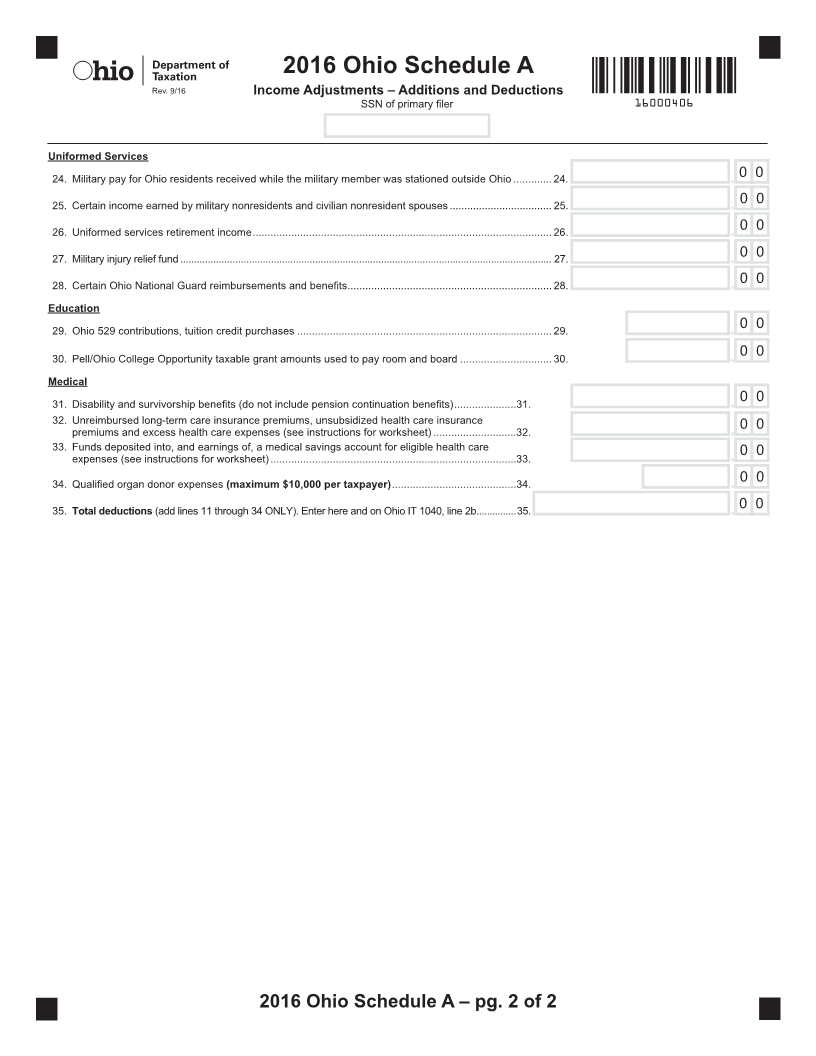
2b.Deductions from federal adjusted gross income (include Ohio Schedule A, line 35).....................2b. . 00
3. Ohio adjusted gross income (line 1 plus line 2a minus line 2b). Place a negative sign (“-“)
before the figure if the amount is less than -0-................................................................................. 3. .00
00
4. Personal and dependent exemption deduction (if claiming dependent(s), include Schedule J)......4. .
5. Ohio income tax base (line 3 minus line 4; if less than -0-, enter -0-)..............................................5. . 00
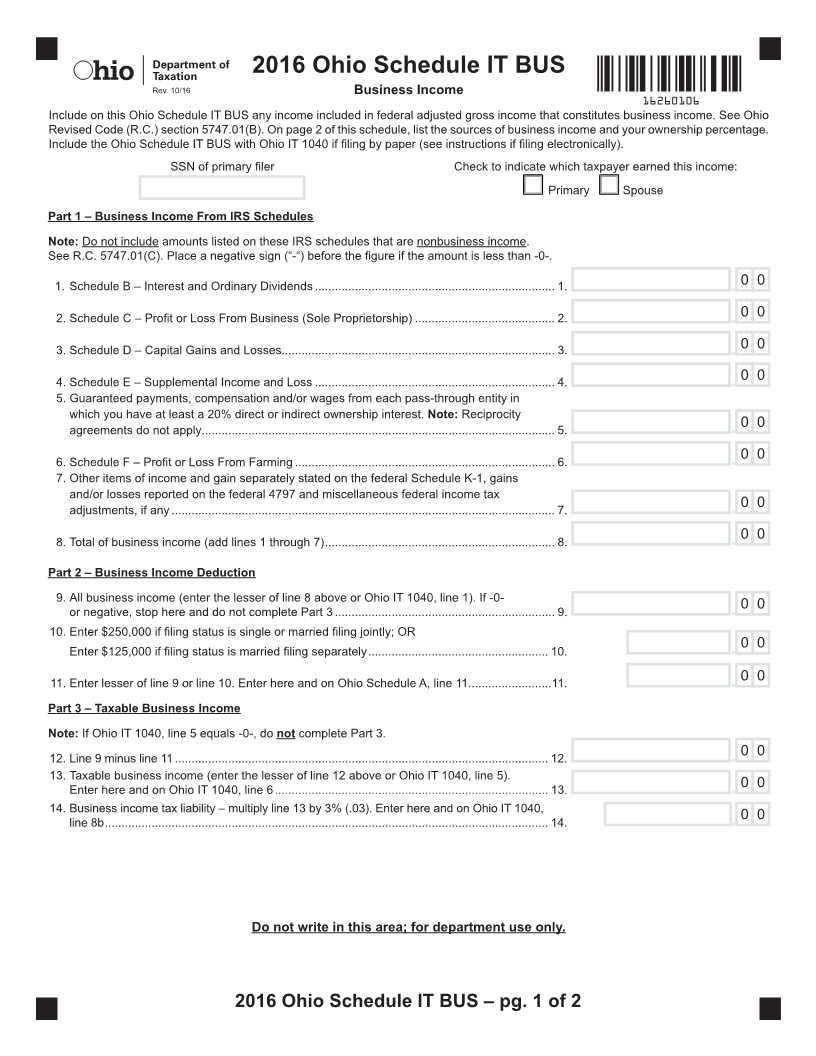
6.Taxable business income (include Ohio Schedule IT BUS, line 13) ................................................ 6. .00
7.Line 5 minus line 6 (if less than -0-, enter -0-).................................................................................. 7. .00
Include your federal income tax return
if line 1 of this return is -0- or negative.
Do not write in this area; for department use only. / /
Postmark date Code
2016 IT 1040 – page 1 of 2
* *