Enlarge image
Use your mouse or Tab key to move through the fields. Use your mouse or space bar to enable check boxes.
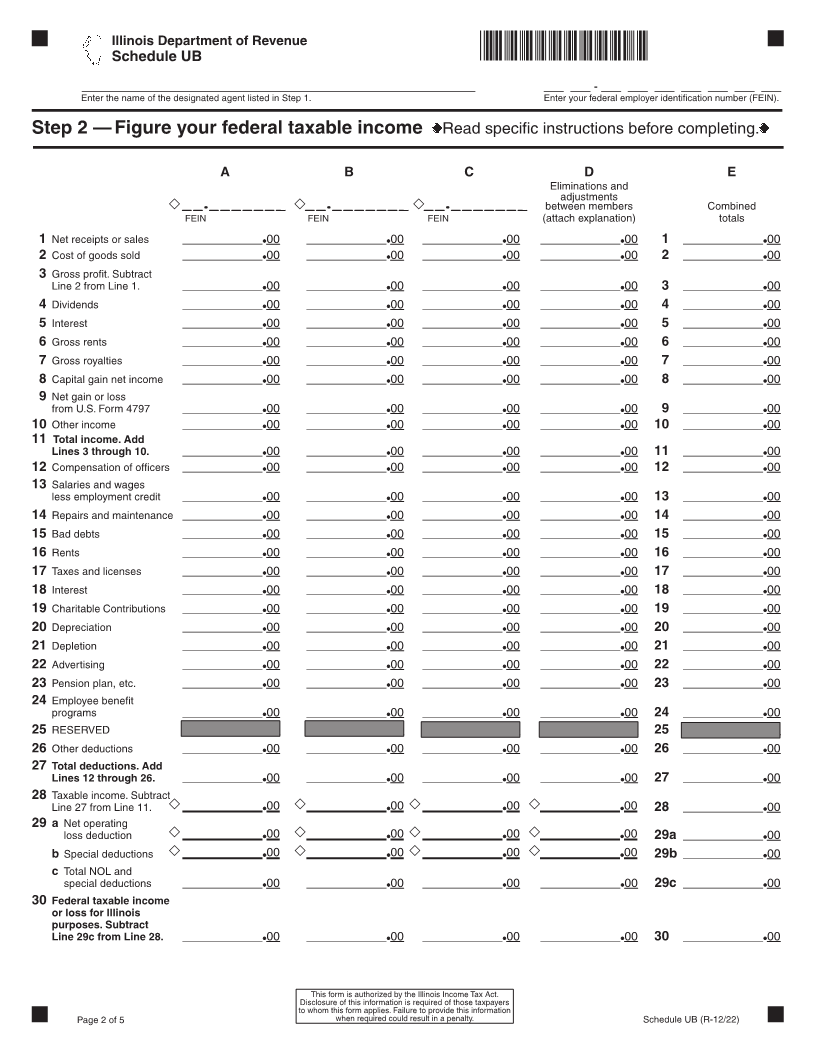
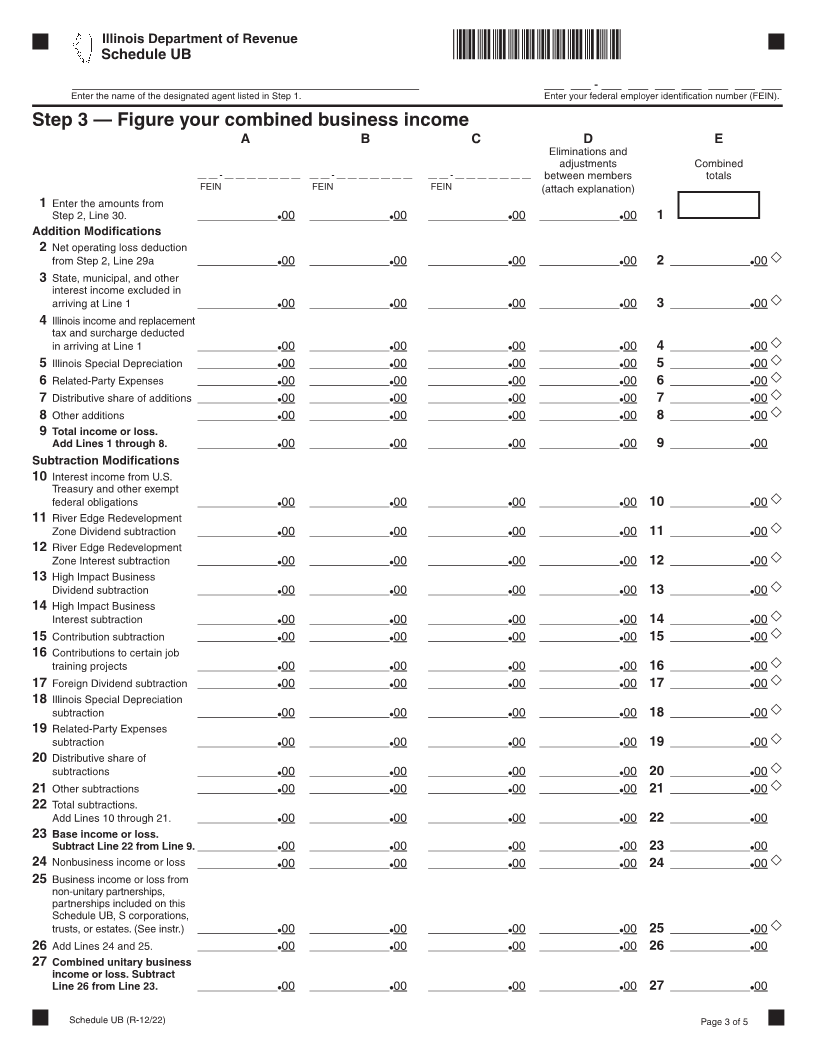
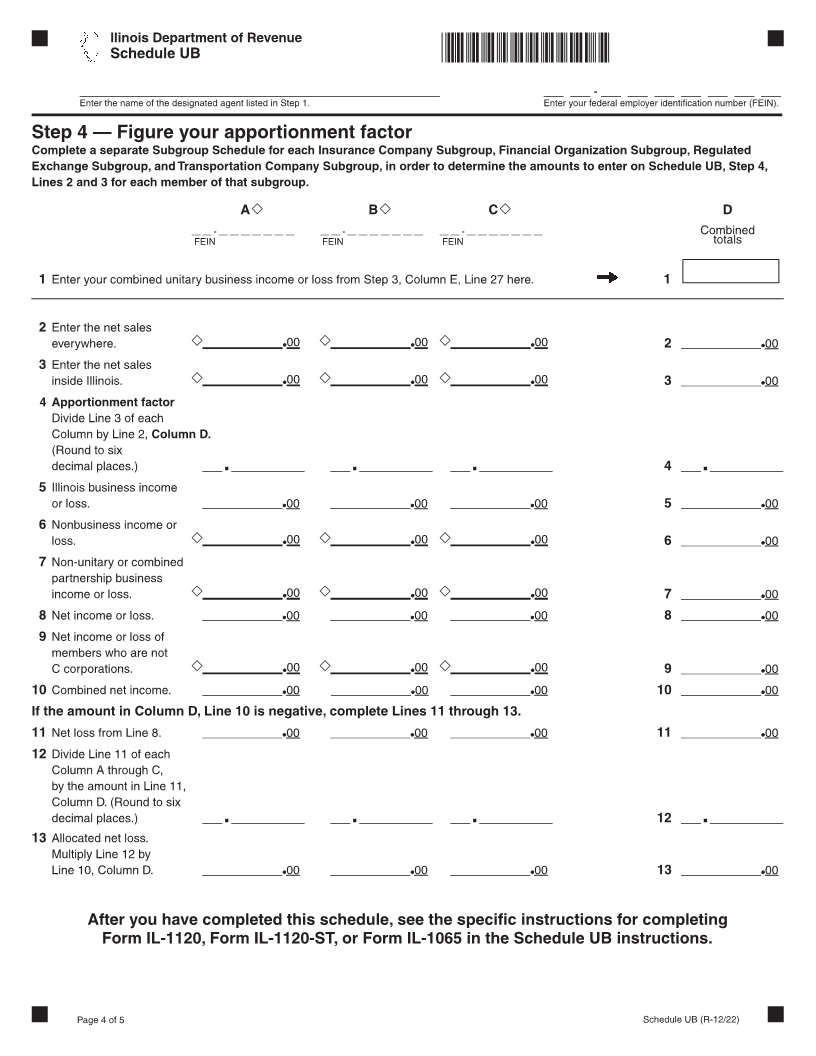
Illinois Department of Revenue
*33312221W* Common year ending for
2022 Schedule UB the unitary business group
Combined Apportionment for Unitary Business Group _____ ____
For tax years ending on or after December 31, 2022. Month Year
Attach to your Form IL-1120, Form IL-1120-ST, or Form IL-1065. IL Attachment No. 5
Step 1 — Provide Your Membership Information
_______________________________________________________________________ _______________________________________________________________________ ___ ___ ______ -- ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___
Enter the name of the designated agent (see general instructions). Enter the federal employer identification number (FEIN).
______________________________________________________________________________________________________________________________________________ ___ ___ ______ -- ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___
Enter the name of the designated agent last year, if it is different than above. Enter the FEIN, if it is different than above.
______________________________________________________________________________________________________________________________________________ ___ ___ ______ -- ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___
Enter the name of the controlling corporation (see general instructions). Enter the FEIN, if it is different than above.
If the controlling corporation is a member of this unitary group, check the box.
Section A — List all members. See Specific Instructions.
A B C D E F G H I
Year Appor-
ending Protected by New Inactive Holding tionment Member
Name FEIN (MM//YYYY) P.L. 86-272 member member company method Type
1____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ _______ _______ / __ _______ _______ __ _____ _____ __________ _____ _____ __________
2____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ _______ _______ / __ _______ _______ __ _____ _____ __________ _____ _____ __________
3____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ _______ _______ / __ _______ _______ __ _____ _____ __________ _____ _____ __________
4 ____________________________________________________________________________________ __ __ - __ __ __ __ __ __ ____ __ __ - __ __ __ __ __ __ ____ __ __ / __ __ __ __ __ __ / __ __ __ __ __________ __________ __________ __________ __________ __________
5 ____________________________________________________________________________________ __ __ - __ __ __ __ __ __ __ __ __ - __ __ __ __ __ __ __ __ __ / __ __ __ ____ __ / __ __ __ __ __________ __________ __________ __________ __________ __________
6____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ _______ _______ / __ _______ _______ __ _____ _____ __________ _____ _____ __________
7____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ ___ _____ __ __ __________ / __ __ ____________ ___ _______________ __________ __________
8____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ ______________ / __ _______ _______ __ __________ __________ _____ _____ __________
9____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ ___ _____ __ __ __________ / __ __ ____________ ___ _______________ __________ __________
10____________________________________________________________________________________ ____ ____ -- ____ ____ ____ ____ ____ ____ ____ __ __ / __ __ __ __ ______________ / __ _______ _______ __ _____ _____ __________ _____ _____ __________
Section B — List any mergers with members listed in Section A. See Specific Instructions.
A B
Person who has merged with member Member listed in Section A
1 ______/________/ / / ________________
Name FEIN Name FEIN Date of merger
2 ________/________/ / /________________
Name FEIN Name FEIN Date of merger
3 ________/________/ / /________________
Name FEIN Name FEIN Date of merger
Section C — List all members who left the group during this tax year. See Specific Instructions.
A B
Member who was sold Entity to which member in Column A was sold
1 ________/________/ / /________________
Name FEIN Name FEIN Date of sale
2 ________/________/ / /________________
Name FEIN Name FEIN Date of sale
3 ________/________/ / /________________
Name FEIN Name FEIN Date of sale
Section D — Provide information about your excluded members
See Specific Instructions and complete Step 5 if the answer below is 1 or greater.
1 Enter the total number of members excluded. ______ ______
Schedule UB (R-12/22) Page 1 of 5