Enlarge image
Use your mouse or Tab key to move through the fields. Use your mouse or space bar to enable check boxes.
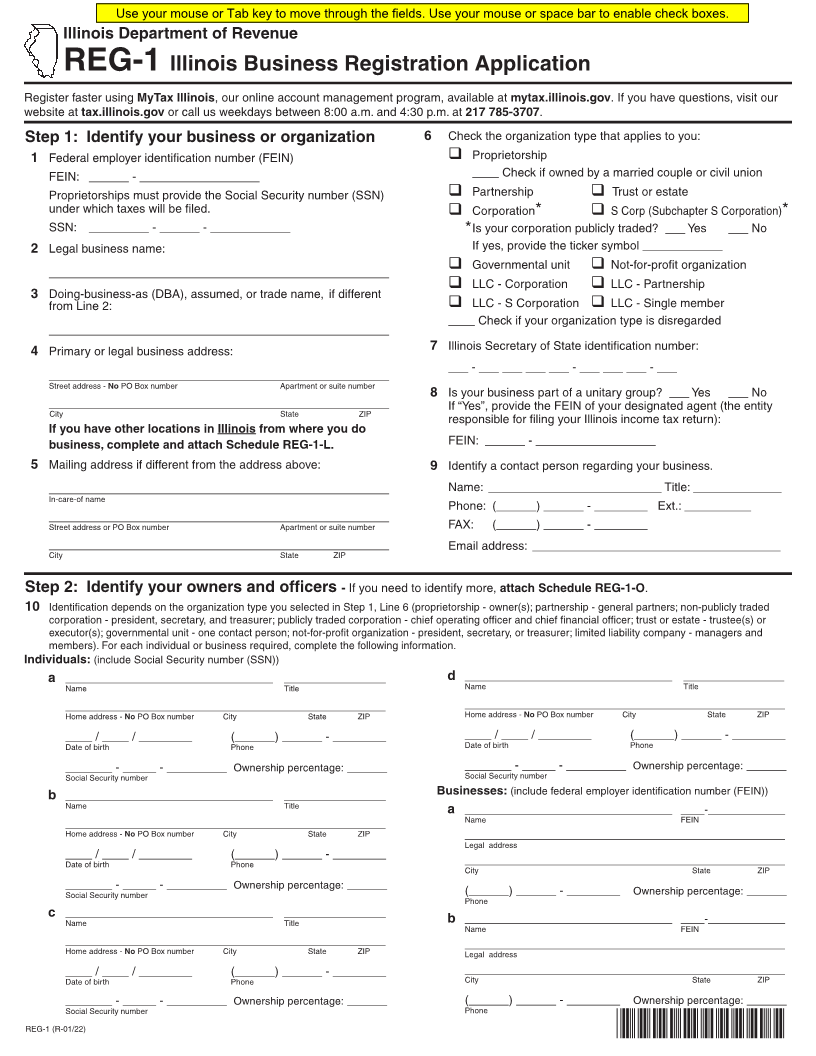
Illinois Department of Revenue
REG-1 Illinois Business Registration Application
Register faster using MyTax Illinois, our online account management program, available at mytax.illinois.gov . If you have questions, visit our
website at tax.illinois.gov or call us weekdays between 8:00 a.m. and 4:30 p.m. at 217 785-3707.
Step 1: Identify your business or organization 6 Check the organization type that applies to you:
1 Federal employer identification number (FEIN) q Proprietorship
FEIN: ______ - __________________ ____ Check if owned by a married couple or civil union
Proprietorships must provide the Social Security number (SSN) q Partnership q Trust or estate
under which taxes will be filed. q Corporation* q S Corp (Subchapter S Corporation)*
SSN: _________ - ______ - ____________ * Is your corporation publicly traded? ___ Yes ___ No
2 Legal business name: If yes, provide the ticker symbol ____________
q Governmental unit q Not-for-profit organization
___________________________________________________
q LLC - Corporation q LLC - Partnership
3 Doing-business-as (DBA), assumed, or trade name, if different
from Line 2: q LLC - S Corporation q LLC - Single member
____ Check if your organization type is disregarded
___________________________________________________
4 Primary or legal business address: 7 Illinois Secretary of State identification number:
___ - ___ ___ ___ ___ - ___ ___ ___ - ___
___________________________________________________
Street address - No PO Box number Apartment or suite number
8 Is your business part of a unitary group? ___ Yes ___ No
___________________________________________________ If “Yes”, provide the FEIN of your designated agent (the entity
City State ZIP
responsible for filing your Illinois income tax return):
If you have other locations in Illinois from where you do
business, complete and attach Schedule REG-1-L. FEIN: ______ - __________________
5 Mailing address if different from the address above: 9 Identify a contact person regarding your business.
___________________________________________________ Name: __________________________ Title: _____________
In-care-of name
Phone: (______) ______ - ________ Ext.: __________
___________________________________________________
Street address or PO Box number Apartment or suite number FAX: (______) ______ - ________
___________________________________________________ Email address: ______________________________________
City State ZIP
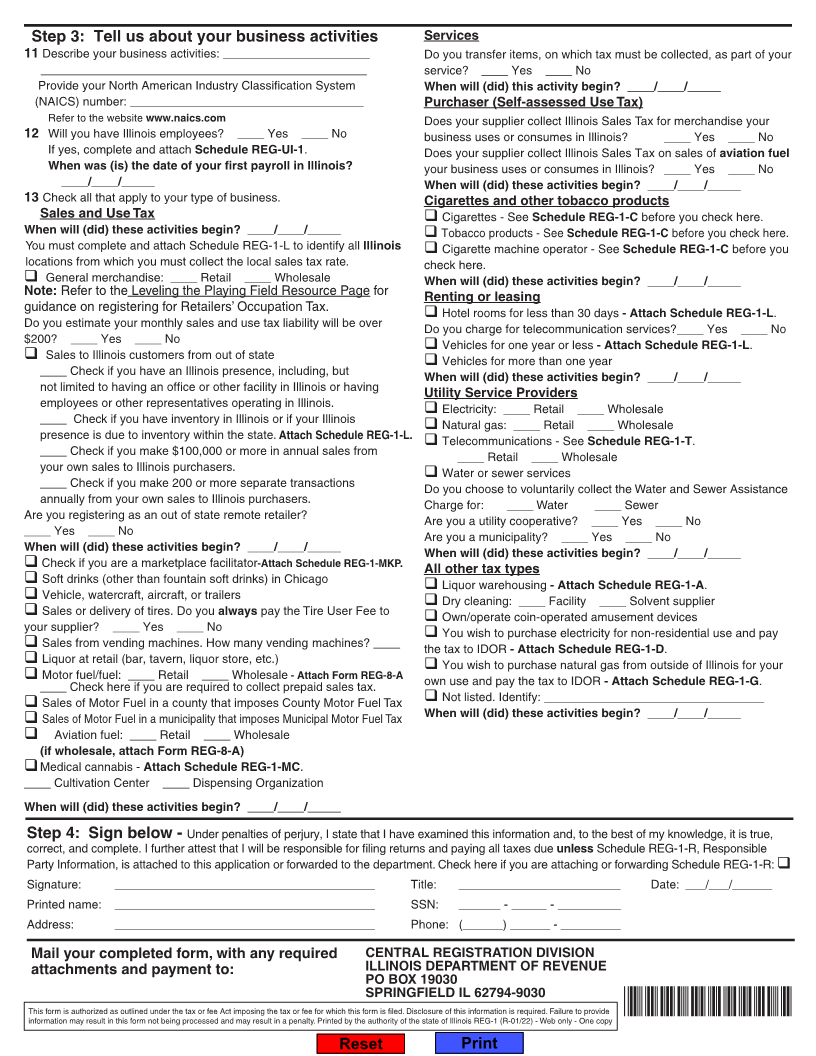
Step 2: Identify your owners and officers - If you need to identify more, attach Schedule REG-1-O.
10 Identification depends on the organization type you selected in Step 1, Line 6 (proprietorship - owner(s); partnership - general partners; non-publicly traded
corporation - president, secretary, and treasurer; publicly traded corporation - chief operating officer and chief financial officer; trust or estate - trustee(s) or
executor(s); governmental unit - one contact person; not-for-profit organization - president, secretary, or treasurer; limited liability company - managers and
members). For each individual or business required, complete the following information.
Individuals: (include Social Security number (SSN))
a ___________________________________ _________________ d ___________________________________ _________________
Name Title Name Title
______________________________________________________ ______________________________________________________
Home address - No PO Box number City State ZIP Home address - No PO Box number City State ZIP
____ / ____ / ________ (______) ______ - ________ ____ / ____ / ________ (______) ______ - ________
Date of birth Phone Date of birth Phone
_______ - _____ - _________ Ownership percentage: ______ _______ - _____ - _________ Ownership percentage: ______
Social Security number Social Security number
b ___________________________________ _________________ Businesses:(include federal employer identification number (FEIN))
Name Title a ___________________________________ ____-_____________
______________________________________________________ Name FEIN
Home address - No PO Box number City State ZIP ______________________________________________________
Legal address
____ / ____ / ________ (______) ______ - ________ ______________________________________________________
Date of birth Phone City State ZIP
_______ - _____ - _________ Ownership percentage: ______ (______) ______ - ________ Ownership percentage: ______
Social Security number Phone
c ___________________________________ _________________ b ___________________________________ ____-_____________
Name Title Name FEIN
______________________________________________________ ______________________________________________________
Home address - No PO Box number City State ZIP Legal address
____ / ____ / ________ (______) ______ - ________ ______________________________________________________
Date of birth Phone City State ZIP
_______ - _____ - _________ Ownership percentage: ______ (______) ______ - ________ Ownership percentage: ______
Social Security number Phone
REG-1 (R-01/22) *74501221W*