Enlarge image
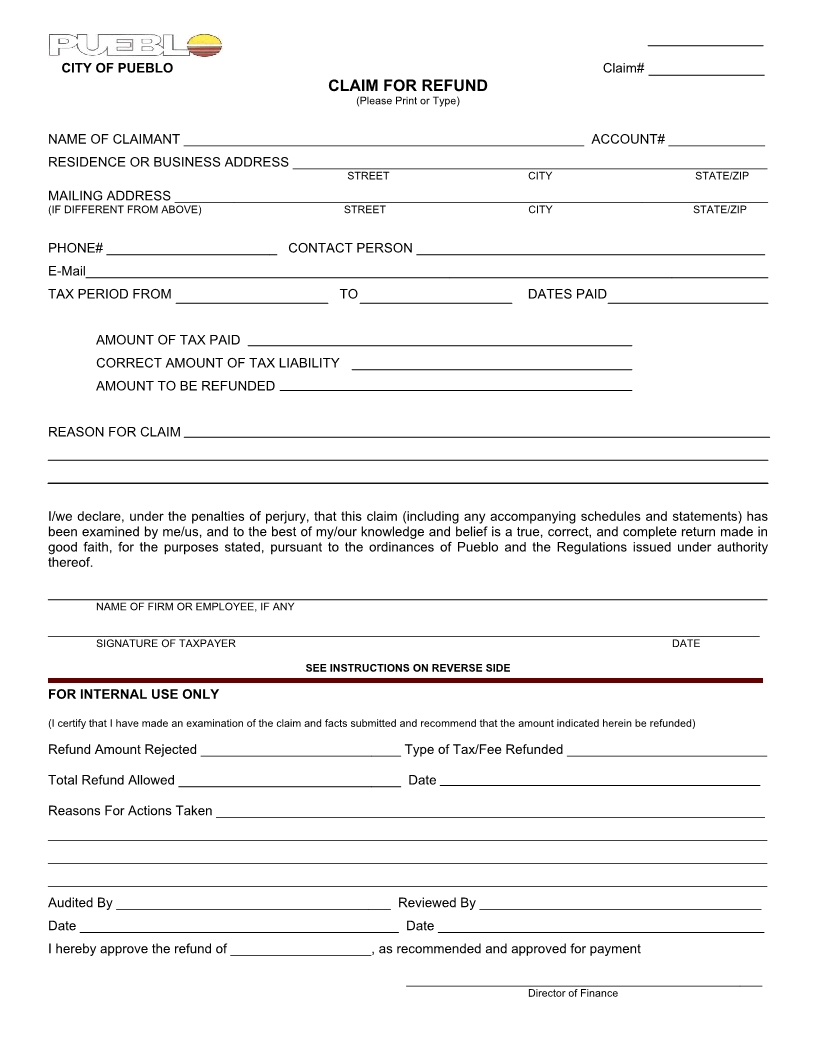
CITY OF PUEBLO _____________Claim#
CLAIM FOR REFUND
(Please Print or Type)
NAME OF CLAIMANT ______________________________________________________ ACCOUNT# _____________
RESIDENCE OR BUSINESS ADDRESS ________________________________________________________________
STREET CITY STATE/ZIP
MAILING ADDRESS ________________________________________________________________________________
(IF DIFFERENT FROM ABOVE) STREET CITY STATE/ZIP
PHONE# _______________________ CONTACT PERSON _______________________________________________
E-Mail____________________________________________________________________________________________
TAX PERIOD FROM TO DATES PAID
AMOUNT OF TAX PAID
CORRECT AMOUNT OF TAX LIABILITY
AMOUNT TO BE REFUNDED
REASON FOR CLAIM
I/we declare, under the penalties of perjury, that this claim (including any accompanying schedules and statements) has
been examined by me/us, and to the best of my/our knowledge and belief is a true, correct, and complete return made in
good faith, for the purposes stated, pursuant to the ordinances of Pueblo and the Regulations issued under authority
thereof.
_________________________________________________________________________________________________
NAME OF FIRM OR EMPLOYEE, IF ANY
________________________________________________________________________________________________________________________
SIGNATURE OF TAXPAYER DATE
SEE INSTRUCTIONS ON REVERSE SIDE
FOR INTERNAL USE ONLY
(I certify that I have made an examination of the claim and facts submitted and recommend that the amount indicated herein be refunded)
Refund Amount Rejected ___________________________ Type of Tax/Fee Refunded ___________________________
Total Refund Allowed ______________________________ Date
Reasons For Actions Taken __________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Audited By _____________________________________ Reviewed By ______________________________________
Date ___________________________________________ Date ____________________________________________
I hereby approve the refund of ___________________, as recommended and approved for payment
________________________________________________
Director of Finance