Enlarge image
1
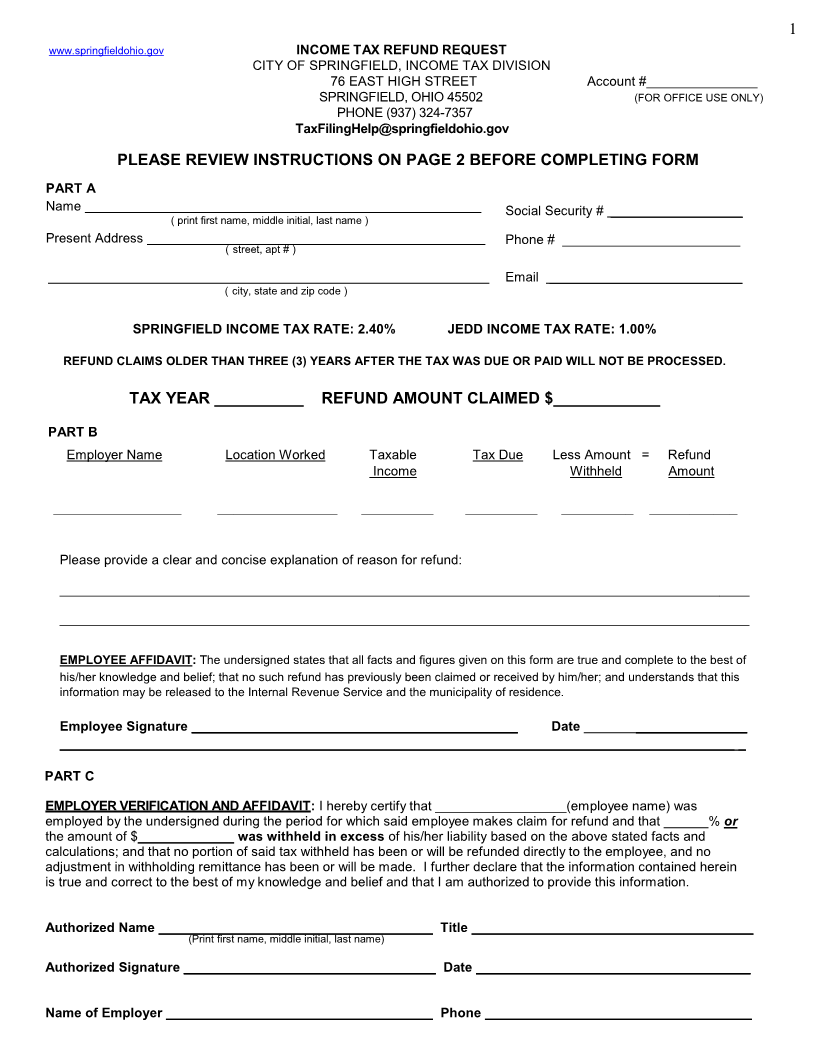
www.springfieldohio.gov INCOME TAX REFUND REQUEST
CITY OF SPRINGFIELD, INCOME TAX DIVISION
76 EAST HIGH STREET Account #_______________
SPRINGFIELD, OHIO 45502 (FOR OFFICE USE ONLY)
PHONE (937) 324-7357
TaxFilingHelp@springfieldohio.gov
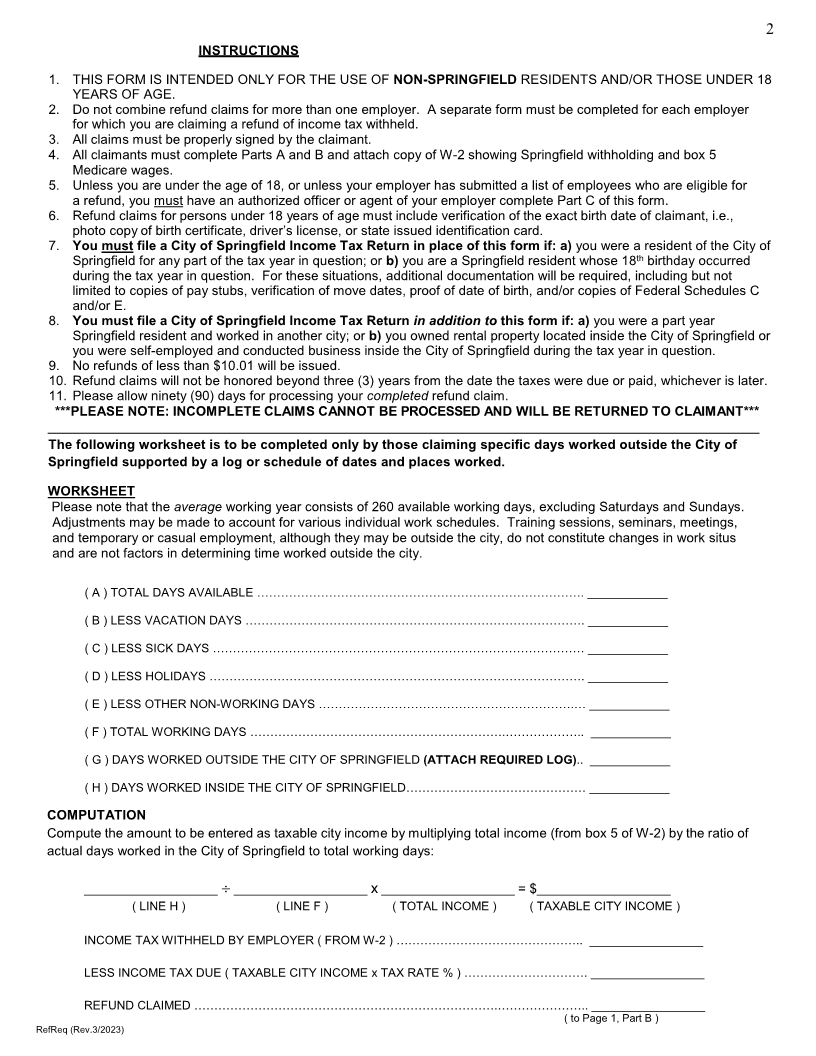
PLEASE REVIEW INSTRUCTIONS ON PAGE 2 BEFORE COMPLETING FORM
PART A
Name Social Security # __________________
( print first name, middle initial, last name )
Present Address Phone # ________________________
( street, apt # )
Email __________________________
( city, state and zip code )
SPRINGFIELD INCOME TAX RATE: 2.40% JEDD INCOME TAX RATE: 1.00%
REFUND CLAIMS OLDER THAN THREE (3) YEARS AFTER THE TAX WAS DUE OR PAID WILL NOT BE PROCESSED.
TAX YEAR __________ REFUND AMOUNT CLAIMED $____________
PART B
Employer Name Location Worked Taxable Tax Due Less Amount = Refund
Income Withheld Amount
________________ _______________ _________ _________ _________ ___________
Please provide a clear and concise explanation of reason for refund:
_____________________________________________________________________________________________
_____________________________________________________________________________________________
EMPLOYEE AFFIDAVIT: The undersigned states that all facts and figures given on this form are true and complete to the best of
his/her knowledge and belief; that no such refund has previously been claimed or received by him/her; and understands that this
information may be released to the Internal Revenue Service and the municipality of residence.
Employee Signature ____________________________________________ Date ______________________
___________________________________________________________________________________________ _
PART C
EMPLOYER VERIFICATION AND AFFIDAVIT: I hereby certify that __________________(employee name) was
employed by the undersigned during the period for which said employee makes claim for refund and that ______% or
the amount of $_____________ was withheld in excess of his/her liability based on the above stated facts and
calculations; and that no portion of said tax withheld has been or will be refunded directly to the employee, and no
adjustment in withholding remittance has been or will be made. I further declare that the information contained herein
is true and correct to the best of my knowledge and belief and that I am authorized to provide this information.
Authorized Name _____________________________________ Title ______________________________________
(Print first name, middle initial, last name)
Authorized Signature __________________________________ Date _____________________________________
Name of Employer ____________________________________ Phone ____________________________________