Enlarge image
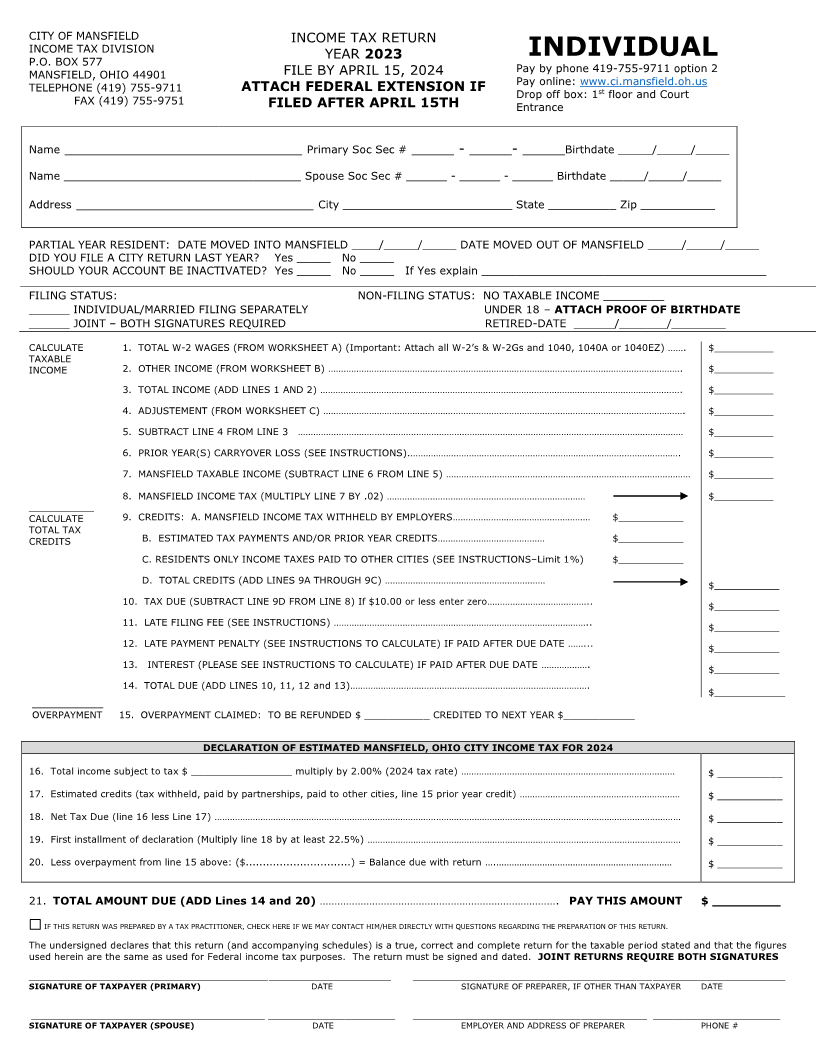
CITY OF MANSFIELD INCOME TAX RETURN
INCOME TAX DIVISION YEAR 2023 INDIVIDUAL
P.O. BOX 577 Pay by phone 419-755-9711 option 2
MANSFIELD, OHIO 44901 FILE BY APRIL 15, 2024
TELEPHONE (419) 755-9711 ATTACH FEDERAL EXTENSION IF Pay online: www.ci.mansfield.oh.us
Drop off box: 1 stfloor and Court
FAX (419) 755-9751 FILED AFTER APRIL 15TH Entrance
Name ____________________________ Primary Soc Sec # _____ - _____- _____Birthdate _____/_____/_____
Name ___________________________________ Spouse Soc Sec # ______ - ______ - ______ Birthdate _____/_____/_____
Address ____________________________ City _________________________ State __________ Zip ___________
PARTIAL YEAR RESIDENT: DATE MOVED INTO MANSFIELD ____/_____/_____ DATE MOVED OUT OF MANSFIELD _____/_____/_____
DID YOU FILE A CITY RETURN LAST YEAR? Yes _____ No _____
SHOULD YOUR ACCOUNT BE INACTIVATED? Yes _____ No _____ If Yes explain __________________________________________
FILING STATUS: NON-FILING STATUS: NO TAXABLE INCOME _________
______ INDIVIDUAL/MARRIED FILING SEPARATELY UNDER 18 – ATTACH PROOF OF BIRTHDATE
______ JOINT –BOTH SIGNATURES REQUIRED RETIRED-DATE ______/_______/________
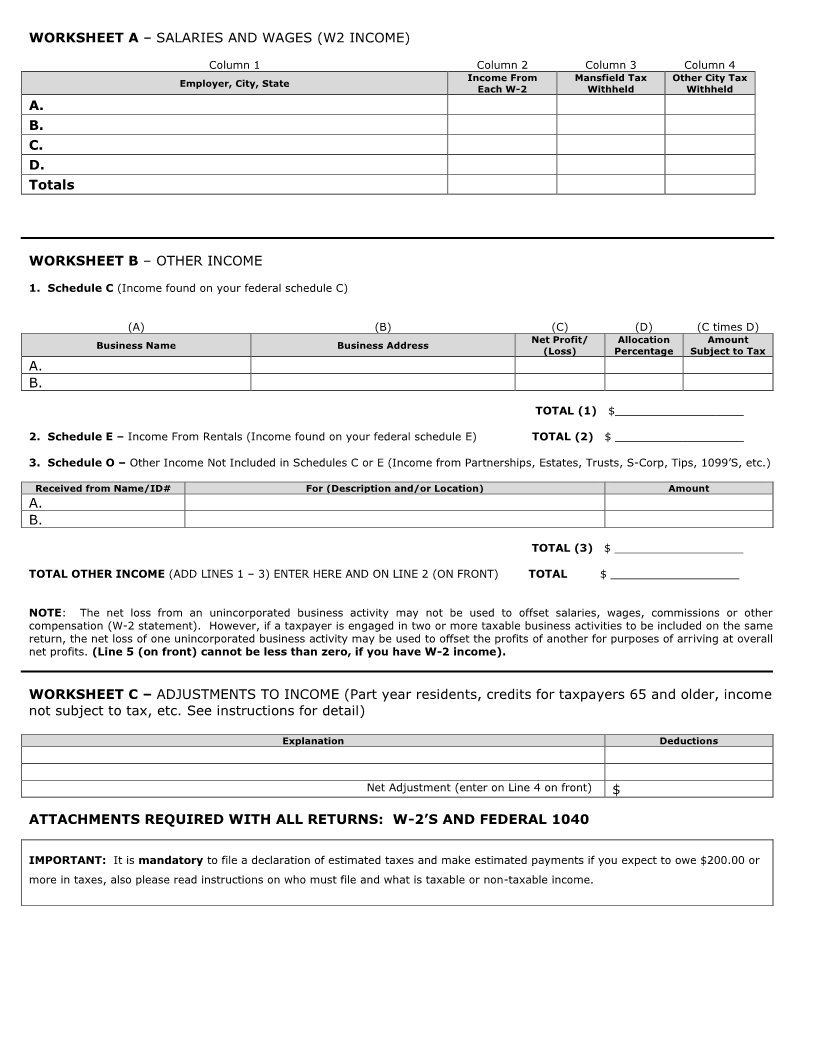
CALCULATE 1. TOTAL W-2 WAGES (FROM WORKSHEET A) (Important: Attach all W-2’s & W-2Gs and 1040, 1040A or 1040EZ) ……. $__________
TAXABLE
INCOME 2. OTHER INCOME (FROM WORKSHEET B) …………………………………………………………………………………………………………………………. $__________
3. TOTAL INCOME (ADD LINES 1 AND 2) ……………………………………………………………………………………………………………………………. $__________
4. ADJUSTEMENT (FROM WORKSHEET C) ……………………………………………………………………………………………………………………………. $__________
5. SUBTRACT LINE 4 FROM LINE 3 …………………………….……………………………………………………………………………………………………… $__________
6. PRIOR YEAR(S) CARRYOVER LOSS (SEE INSTRUCTIONS).……………………………………………………………………………………………. $__________
7. MANSFIELD TAXABLE INCOME (SUBTRACT LINE 6 FROM LINE 5) …………………………………………………………………………………… $__________
8. MANSFIELD INCOME TAX (MULTIPLY LINE 7 BY .02) …………………………………………………………………… $__________
___________
CALCULATE 9. CREDITS: A. MANSFIELD INCOME TAX WITHHELD BY EMPLOYERS……………………………………………… $___________
TOTAL TAX
CREDITS B. ESTIMATED TAX PAYMENTS AND/OR PRIOR YEAR CREDITS…………………………………… $___________
C. RESIDENTS ONLY INCOME TAXES PAID TO OTHER CITIES (SEE INSTRUCTIONS–Limit 1%) $___________
D. TOTAL CREDITS (ADD LINES 9A THROUGH 9C) ……………………………………………………… $___________
10. TAX DUE (SUBTRACT LINE 9D FROM LINE 8) If $10.00 or less enter zero………………………………….. $___________
11. LATE FILING FEE (SEE INSTRUCTIONS) ……………………………………………………………………………………….. $___________
12. LATE PAYMENT PENALTY (SEE INSTRUCTIONS TO CALCULATE) IF PAID AFTER DUE DATE ……... $___________
13. INTEREST (PLEASE SEE INSTRUCTIONS TO CALCULATE) IF PAID AFTER DUE DATE ……………….
$___________
14. TOTAL DUE (ADD LINES 10, 11, 12 and 13)………………………………………………………………………………….
$____________
____________
OVERPAYMENT 15. OVERPAYMENT CLAIMED: TO BE REFUNDED $ ___________ CREDITED TO NEXT YEAR $____________
DECLARATION OF ESTIMATED MANSFIELD, OHIO CITY INCOME TAX FOR 2024
16. Total income subject to tax $ _________________ multiply by 2.00% (2024 tax rate) ………………………………………………………………………… $ ___________
17. Estimated credits (tax withheld, paid by partnerships, paid to other cities, line 15 prior year credit) ……………………………………………………… $ ___________
18. Net Tax Due (line 16 less Line 17) ………………………………………………………………………………………………………………………………………………………………… $ ___________
19. First installment of declaration (Multiply line 18 by at least 22.5%) …………………………………………………………………………………………………………… $ ___________
20. Less overpayment from line 15 above: ($...............................) = Balance due with return ….…………………………………………………………… $ ___________
21. TOTAL AMOUNT DUE (ADD Lines 14 and 20) ………………………………………………………………………. PAY THIS AMOUNT $ _________
IF THIS RETURN WAS PREPARED BY A TAX PRACTITIONER, CHECK HERE IF WE MAY CONTACT HIM/HER DIRECTLY WITH QUESTIONS REGARDING THE PREPARATION OF THIS RETURN.
The undersigned declares that this return (and accompanying schedules) is a true, correct and complete return for the taxable period stated and that the figures
used herein are the same as used for Federal income tax purposes. The return must be signed and dated. JOINT RETURNS REQUIRE BOTH SIGNATURES
_______________________________________________ ________________________ _______________________________________________ __________________________
SIGNATURE OF TAXPAYER (PRIMARY) DATE SIGNATURE OF PREPARER, IF OTHER THAN TAXPAYER DATE
______________________________________________ _________________________ ______________________________________________ _________________________
SIGNATURE OF TAXPAYER (SPOUSE) DATE EMPLOYER AND ADDRESS OF PREPARER PHONE #