Enlarge image
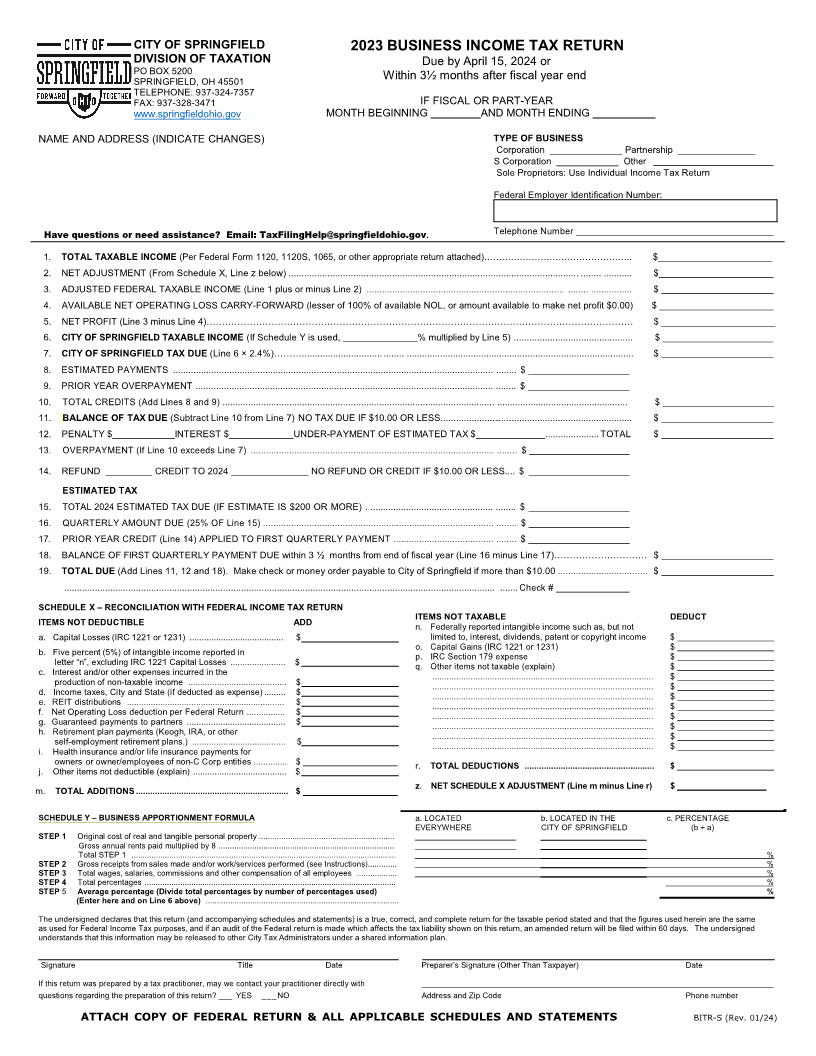
CITY OF SPRINGFIELD 202 3BUSINESS INCOME TAX RETURN
DIVISION OF TAXATION Due by April 15, 2024or
PO BOX 5200 Within 3½ months after fiscal year end.
SPRINGFIELD, OH 45501
TELEPHONE: 937-324-7357
FAX: 937-328-3471 IF FISCAL OR PART-YEAR
www.springfieldohio.gov MONTH BEGINNING AND MONTH ENDING
NAME AND ADDRESS (INDICATE CHANGES) TYPE OF BUSINESS
Corporation ______________ Partnership _______________
S Corporation ____________ Other
Sole Proprietors: Use Individual Income Tax Return
Federal Employer Identification Number:
Have questions or need assistance? Email: TaxFilingHelp@springfieldohio.gov. Telephone Number
1. TOTAL TAXABLE INCOME (Per Federal Form 1120, 1120S, 1065, or other appropriate return attached)………………………………………….. $______________________
2. NET ADJUSTMENT (From Schedule X, Line z below) ................................................................................................................ ........ ........... $
3. ADJUSTED FEDERAL TAXABLE INCOME (Line 1 plus or minus Line 2) ............................................................................. ........ ................ $
4. AVAILABLE NET OPERATING LOSS CARRY-FORWARD (lesser of 100% of available NOL, or amount available to make net profit $0.00) $ ______________________
5. NET PROFIT ( ineL 3 minus Line 4)………………………………………………………………………………………………………………………… $ ______________________
6. CITY OF SPRINGFIELD TAXABLE INCOME (If Schedule Y is used, % multiplied by Line 5) .............................................. $ _____________________
7. CITY OF SPRINGFIELD TAX DUE (Line 6 × 2.4%)………............................... ........ ........................................................................................ $
8. ESTIMATED PAYMENTS ............................................................................................................................. ........ $
9. PRIOR YEAR OVERPAYMENT .................................................................................................................... ........ $
10. TOTAL CREDITS (Add Lines 8 and 9) .......................................................................................................... ................................................... $ _____________________
11. BALANCE OF TAX DUE (Subtract Line 10 from Line 7) NO TAX DUE IF $10.00 OR LESS........................................................................... $
12. PENALTY $ INTEREST $ UNDER-PAYMENT OF ESTIMATED TAX $ ..................... TOTAL $
13. OVERPAYMENT (If Line 10 exceeds Line 7) ............................................................................................... ........ $
14. REFUND _________ CREDIT TO 202 4_______________ NO REFUND OR CREDIT IF $10.00 OR LESS .... $
ESTIMATED TAX
15. TOTAL 2024ESTIMATED TAX DUE (IF ESTIMATE IS $200 OR MORE) . ................................................ ........ $
16. QUARTERLY AMOUNT DUE (25% OF Line 15) .......................................................................................... ........ $
17. PRIOR YEAR CREDIT (Line 14) APPLIED TO FIRST QUARTERLY PAYMENT ....................................... ........ $
18. BALANCE OF FIRST QUARTERLY PAYMENT DUE within 3 ½ months from end of fiscal year (Line 16 minus Line 17)………………………… $
19. TOTAL DUE (Add Lines 11, 12 and 18). Make check or money order payable to City of Springfield if more than $10.00 ................................... $
........................................................................................................................................................................ ....... Check #
SCHEDULE X – RECONCILIATION WITH FEDERAL INCOME TAX RETURN
ITEMS NOT DEDUCTIBLE ADD ITEMS NOT TAXABLE DEDUCT
n. Federally reported intangible income such as, but not
a. Capital Losses (IRC 1221 or 1231) ....................................... $ limited to, interest, dividends, patent or copyright income $
b. Five percent (5%) of intangible income reported in o. Capital Gains (IRC 1221 or 1231) $
letter “n”, excluding IRC 1221 Capital Losses ....................... $ p. IRC Section 179 expense $
c. Interest and/or other expenses incurred in the q. Other items not taxable (explain) $
production of non-taxable income ......................................... $ ............................................................................................ $
d. Income taxes, City and State (if deducted as expense) ......... $ ............................................................................................ $
e. REIT distributions .................................................................. $ ............................................................................................ $
f. Net Operating Loss deduction per Federal Return ................ $ ............................................................................................ $
g. Guaranteed payments to partners ......................................... $ ............................................................................................ $
h. Retirement plan payments (Keogh, IRA, or other ............................................................................................ $
self-employment retirement plans.) ....................................... $ ............................................................................................ $
i. Health insurance and/or life insurance payments for ............................................................................................ $
owners or owner/employees of non-C Corp entities .............. $ r. TOTAL DEDUCTIONS ...................................................... $
j. Other items not deductible (explain) ....................................... $
m. TOTAL ADDITIONS ................................................................ $ z. NET SCHEDULE X ADJUSTMENT (Line m minus Line r) $ ___________________
SCHEDULE Y – BUSINESS APPORTIONMENT FORMULA a. LOCATED b. LOCATED N I THE c. PERCENTAGE
EVERYWHERE CITY OF SPRINGFIELD (b ÷ a)
STEP 1 Original cost of real and tangible personal property .............................................................
Gross annual rent s paid multiplied by ...............................................................................8
Total STEP 1 ....................................................................................................................... %
STEP 2 Gross receipts from sales made and/or work/services performed (see Instructions)............. %
STEP 3 Total wages, salaries, commissions and other compensation of all employees .................. %
STEP 4 Total percentages ................................................................................................................. %
STEP 5 Average percentage (Divide total percentages by number of percentages used) %
(Enter here and on Line 6 above) .......................................................................................
The undersigned declares that this return (and accompanying schedules and statements) is a true, correct, and complete return for the taxable period stated and that the figures used herein are the same
as used for Federal Income Tax purposes, and if an audit of the Federal return is made which affects the tax liability shown on this return, an amended return will be filed within 60 days. The undersigned
understands that this information may be released to other City Tax Administrators under a shared information plan.
Signature Title Date Preparer’s Signature (Other Than Taxpayer) Date
If this tre urn was prepared by ta ax practitioner,may we con act yourt prac itionert direc lyt wit h
questions regarding the preparation of this return? ___ YES ___NO Address and Zip Code Phone number
ATTACH COPY OF FEDERAL RETURN & ALL APPLICABLE SCHEDULES AND STATEMENTS BITR-S (Rev. 01/24)