Enlarge image
INCOME TAX DIVISION Telephone: 330-375-2290
Fax: 330-375-2112
DEPARTMENT OF FINANCE
Email: incometax@akronohio.gov
www.akronohio.gov/1040
1 Cascade Plaza - Suite 100
Akron, Ohio 44308-1161
Donald W Smith, CPA
Tax Commissioner
Dear Taxpayer,
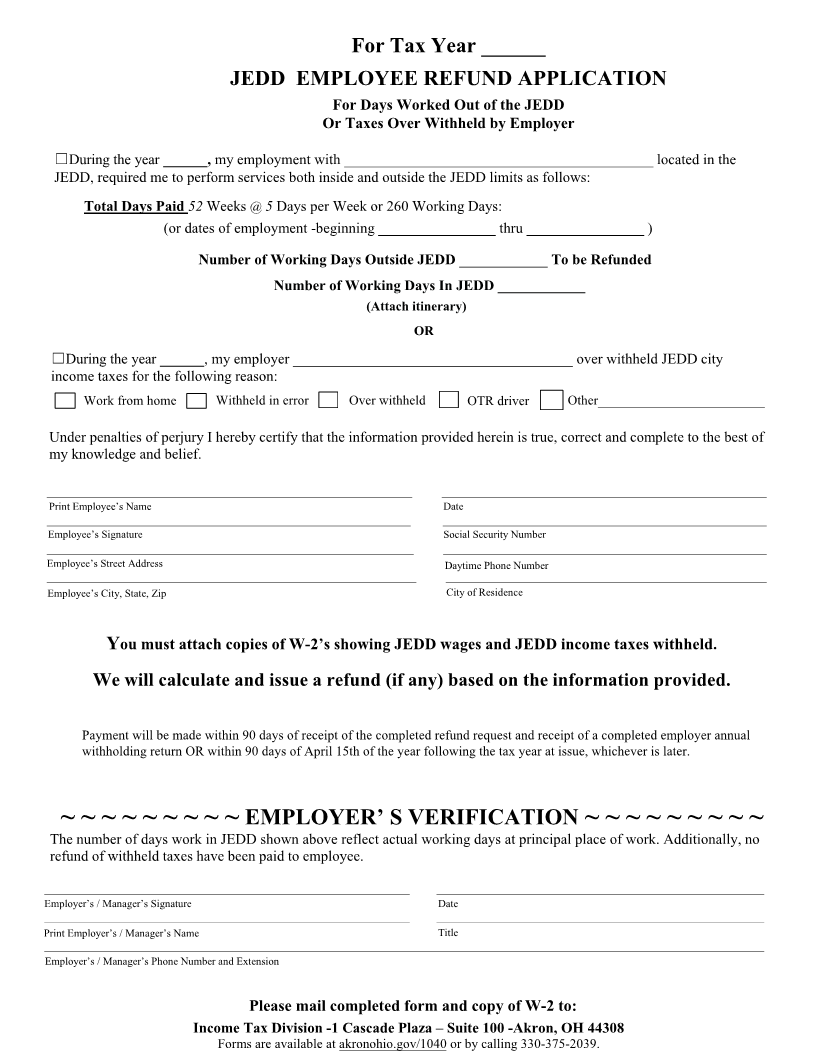
Use the Non-Resident Employee Refund Application if your request is for
days worked outside of Akron. You must complete the entire form. Then have
the days worked in Akron verified for accuracy by your employer. (The
appropriate individual is one who has legal authority to sign for the company
and knows your work schedule.)
In addition, please be advised that we will be notifying your resident city. It
appears that one of the intentions of the new State law is to hold the employee
responsible to pay either the city where the work was performed or the base
city of employment, when both are taxing municipalities. Since you are
receiving a refund of taxes withheld for your base city of employment, the city
of residence may elect to pursue recovery of these dollars.
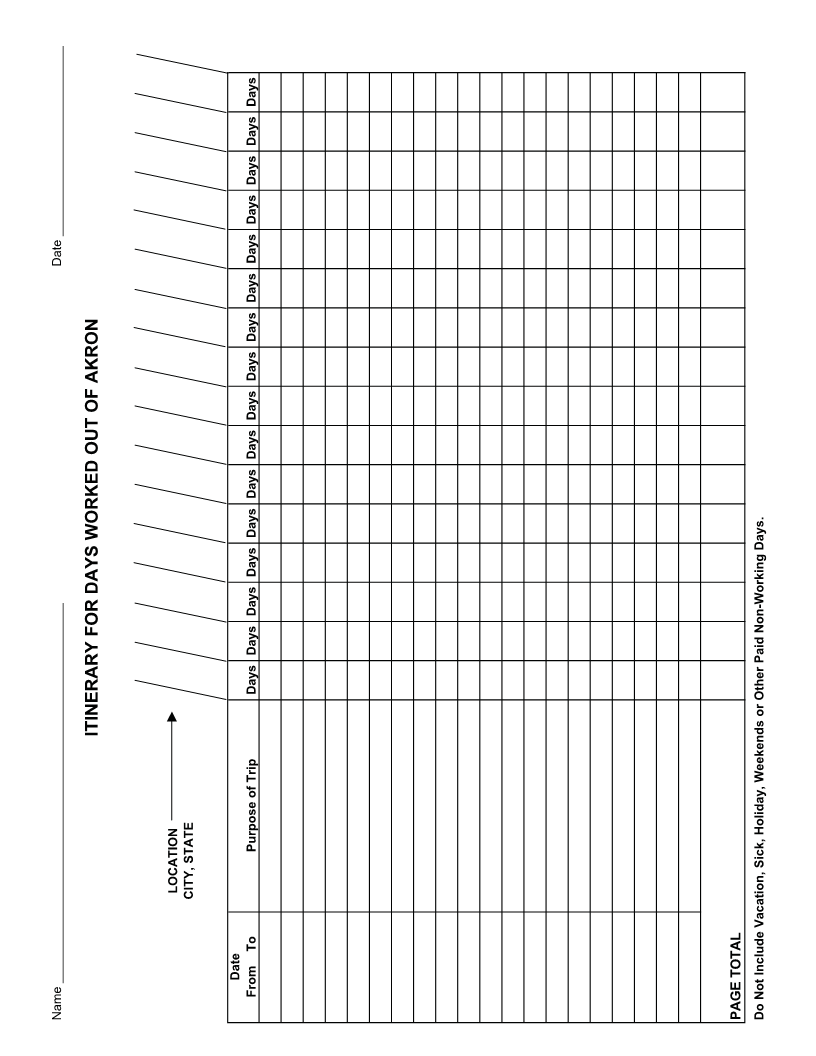
Refunds are issued within 90 days after the City has receipt of the correctly
completed Refund Application and itinerary forms, or after receipt of the
employer’s correct AW-3 reconciliation form, including all W-2 information,
whichever is later.
Sincerely,
Income Tax Division
Refund Section
330-375-2039
Revised: 1/2024