Enlarge image
CITY OF SPRINGFIELD FORM W-1
INCOME TAX DIVISION
76 E.HIGH STREET FORM W-3
SPRINGFIELD OH 45502
(937) 324-7357
EMPLOYER CITY TAX WITHHOLDING BOOKLET
FOR TAX YEARS 2018 AND FORWARD
Questions or Concerns? Email: TaxFilingHelp@springfieldohio.gov
NOTE TO EMPLOYERS
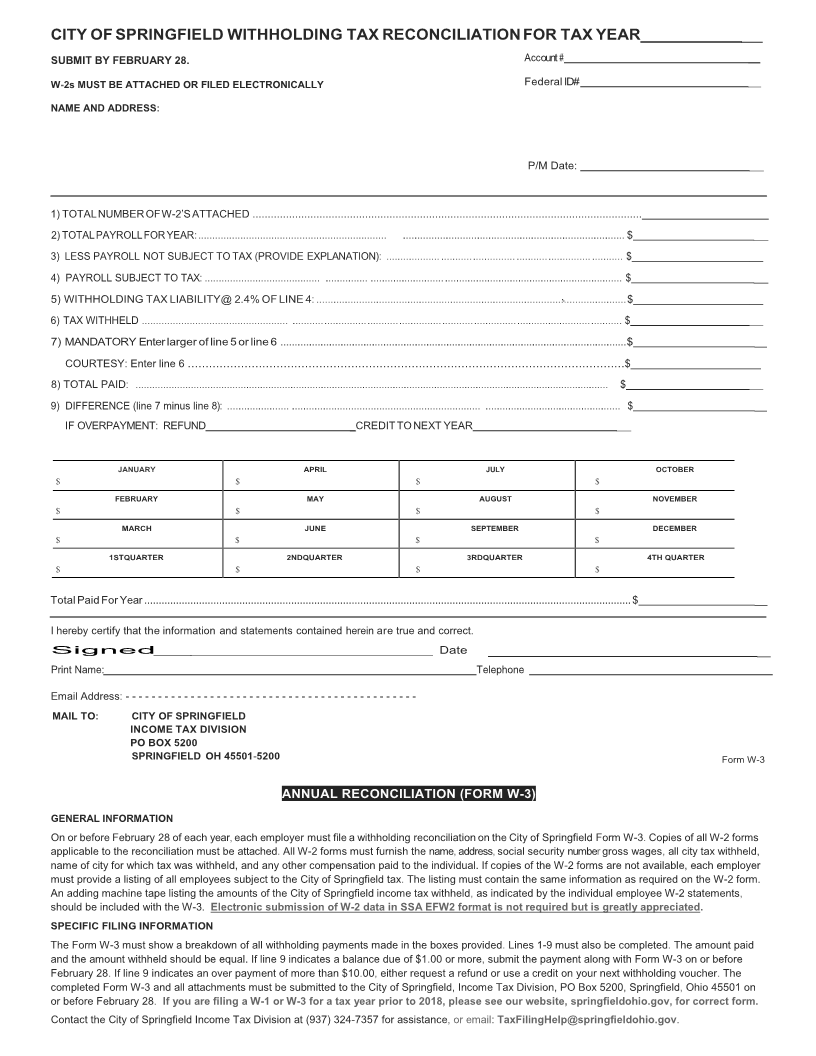
These forms are to be used for the filing of withholding payments The. W-1 forms can be used for either monthly or quarterly periods The W-3. is for the
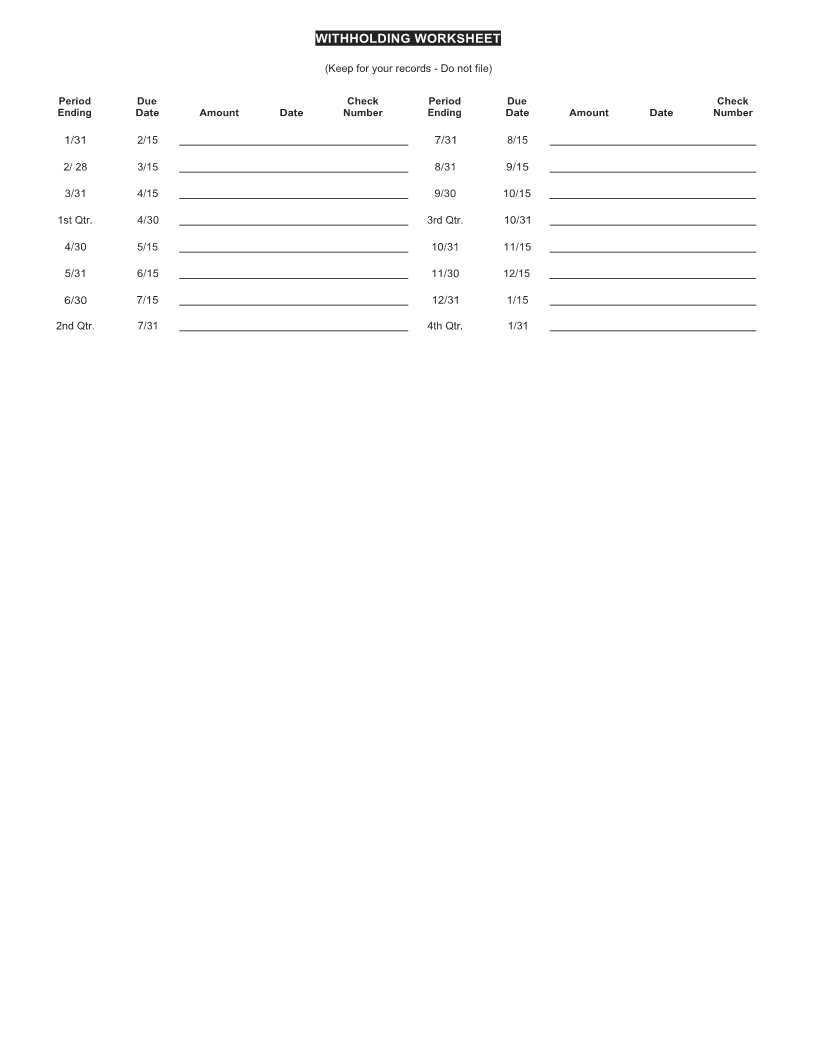
year end reconciliation Also. included is a summary worksheet for your records If you. have any questions, you may contact our office at (937) 324-7357.
Additional forms and information are available on the City of Springfield website at www springfieldohio. gov.If required. to make Federal withholding tax
payments electronically,you are also required to pay Springfield withholding taxes by electronic funds transfer You. may file and pay electronically using 3
different options:
1. Tax Connect on the city website (or go directly to: https://web1.civicacmi.com/SpringfieldTax/)
2. Ohio Business Gateway
3. ACH Credit - using your own template and software Contact. the City of Springfield Income Tax Division for
details.
GENERAL INFORMATION
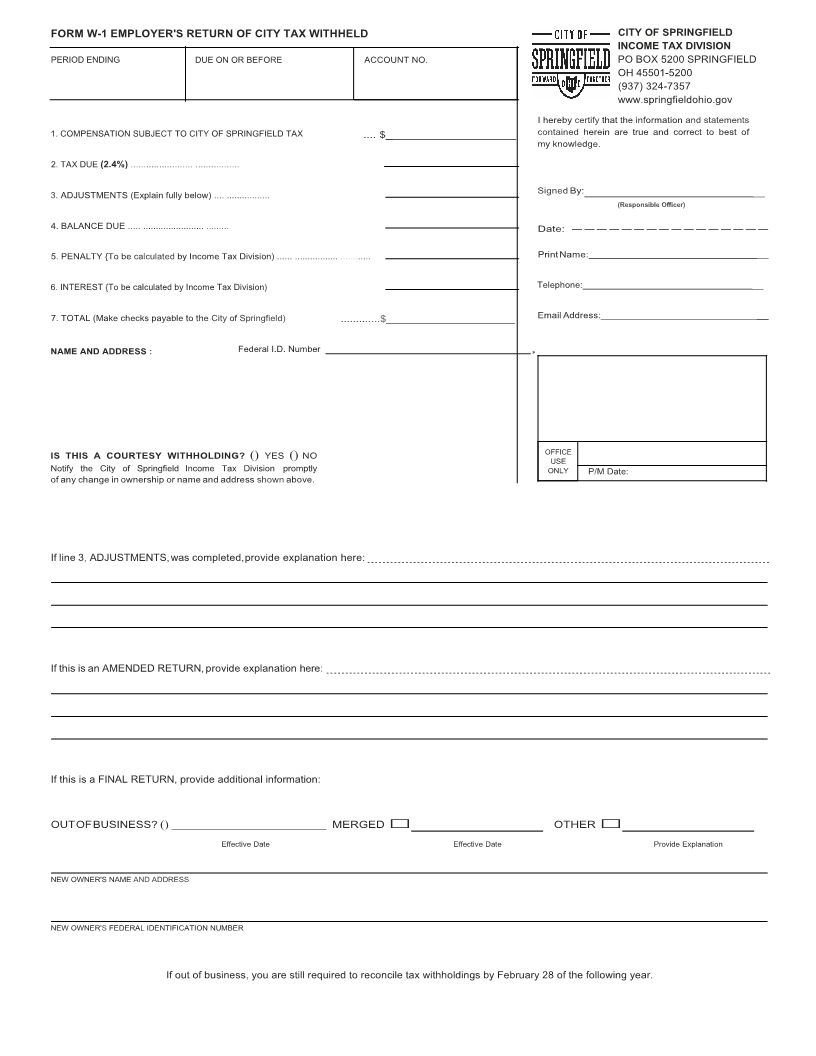
Each employer located within or doing business within the City of Springfield who employs one or more persons, is required to withhold the City of
Springfield income tax at the rate of 2 4%. from all compensation allocated or set aside for or paid, to the,employee(s ) Each.employer is required to file
the Employer’s Return of City Tax Withheld (Form W-1) along with the monthly, semi-monthly or quarterly withholding payments on or before the due
dates as shown below The. failure of any employer to receive or procure Form W-1 shall not excuse him/her from making this return or from remitting the
tax withheld.Per ORC 718, for tax years 2017 and forward :
THRESHOLD
1. Monthly remittance is required if the total Springfield withholding during the preceding calendar year exceeded $2,399 00; or. any month of the
preceding quarter exceeded $200 00. .
2. Semi-monthly remittance may be required if the total Springfield withholding during the preceding calendar year exceeded $11,999 00; or. any month
of the preceding calendar year exceeded $1 000, 00. .
3. Quarterly remittance is allowed when monthly or semi-monthly remittance is not required.
DUE DATES
1. Monthly - due by the 15th day of the next month .
2. Quarterly - due by the last day of the month following the end of the quarter.
3. Semi-monthly - taxes withheld during the first 15 days of a month are due by the 3rd banking day after the 15th of the month Taxes. withheld after
the 15th of the month to the end of the month are due by the 3rd banking day after the last day of the month.
FORM W-1 FILING INSTRUCTIONS
LINE 1 Enter the total compensation allocated, set aside, or paid to all taxable employees during the filing period If no.compensation was
allocated,set aside or, paid during this period record, a zero (0) on lines 1-7 and return Form W-1 to the City of Springfield Income, Tax
Division.
LINE 2 Compute tax due (2. 4%. times payroll).
LINE 3 Enter any adjustments to the tax withheld on line 2; e g.additional., tax withheld at employee request, other city payments, etc All .
adjustments must be explained.
LINE 4 Amount of tax due must be paid with this return.
LINES 5 &6 Penalty and Interest on late payments will be calculated by the City of Springfield Income Tax Division .
LINE 7 Tax due plus penalty and interest, if applicable.
The Name,Address, Federal Identification Number and Responsible Officer's information must be provided for the return to be complete .
PENALTY AND INTEREST
Payment and Form W-1 not received on or before the due date shall be considered delinquent and shall be subject to penalty and interest charges as
provided for in the City of Springfield Tax Ordinance. Contact the City of Springfield, Income Tax Division (937), 324-7357 for the applicable charges .
TAX YEARS 2017 AND FORWARD
Late Payment Penalty: up to 50% of tax due
Interest: For the applicable tax year, the federal short-term rate rounded to the nearest whole number percent, plus five percent
Late Filing Penalty: $25.00 per late month